![]()
![]()
Mustafa KorkutI; Cihan BedelI; Ramazan SivilI; Mücahit Alp ArslanII; Fatih SelviI; Görkem KuşIII; Ökkeş ZortukI
DOI: 10.21470/1678-9741-2021-0088
ABSTRACT
Objective: ST-segment elevation myocardial infarction (STEMI) is a serious, life-threatening disease. Inflammatory markers have recently become the focus of attention in the assessment of severity in the early stages of STEMI. This study aimed to evaluate the importance of immature granulocytes (IG) as a prognostic marker in STEMI.ALT= Alanine transaminase
BUN= Blood urea nitrogen
CBC= Complete blood count
CRP= C-reactive protein
DBP= Diastolic blood pressure
EF= Ejection fraction
Hb= Hemoglobin
HDL= High-density lipoprotein
hsTnT= High-sensitive troponin-T
IG= Immature granulocytes
LDL= Low-density lipoprotein
LVEF= Left ventricular ejection fraction
MI= Myocardial infarction
MPV= Mean platelet volume
NLR= Neutrophil-lymphocyte ratio
NT-proBNP= N-terminal pro-brain natriuretic peptide
OR= Odds ratio
Plt= Platelets
pPCI= Primary percutaneous coronary intervention
ROC= Receiver operating characteristic
HT= Hypertension
SBP= Systolic blood pressure
STEMI= ST-segment elevation myocardial
INTRODUCTION
ST-segment elevation myocardial infarction (STEMI) is caused by a blockage in the coronary arteries and, as a result, interruption of blood flow to the myocardium[1,2]. Despite the significant improvements achieved so far through modern technological advances and revascularization techniques, medical treatments and secondary prevention measures, STEMI remains a major cause of mortality not only in our country, Turkey, but also in the world[3]. In-hospital mortality and potential prognostic indicators after a myocardial disease have been investigated in many studies[4]. Advancing age, neutrophil-lymphocyte ratio (NLR), and serum creatinine levels have been reported to have a significant correlation with in-hospital and short-term mortality. In STEMI, an excessive inflammatory response occurs as a result of early ischaemia. Therefore, inflammatory markers have recently become the focus of attention in the assessment of severity in the early stages of STEMI[5,6].
The immature granulocytes (IG) count, which is a practical marker of local and systemic inflammation, can be quickly and easily obtained using a complete blood count (CBC) by means of recent technological advances such as automated blood cell analysers. The IG count can reflect the fraction of circulating IG without demanding extra costs or time[7-9]. A literature review has shown that only a few studies have investigated the association between the IG count and the severity of STEMI. Therefore, this study aimed to evaluate the significance of the IG count as a prognostic marker in STEMI.
METHODS
Ethics committee approval was obtained with decision date and number was 1/10/2020 and 15/6 before starting the study. Data from patients who were admitted to the emergency department with chest pain, admitted in the coronary care unit with a STEMI diagnosis, and who underwent primary percutaneous coronary intervention (pPCI) within the period from January 1st 2019 to January 1st 2020, were reviewed retrospectively. The respective data were retrieved and documented from the hospital automation system file. Criteria provided by international cardiology societies were used to make the diagnosis of STEMI[10]. Patients’ age, gender, haemogram, biochemistry results and mortality were recorded. A total of 146 patients aged ≥18 years meeting the study inclusion criteria were enrolled in the study. Patients under 18 years old, pregnant women, patients with myeloproliferative and chronic inflammatory diseases, kidney disease, liver disease, and malignancies, patients with missing information in medical records, patients referred to an external centre, and patients who refused treatment were excluded from the study. Twenty-one patients were excluded from the study as per the above criteria.
All patients included in the study underwent pPCI as an indicator of revascularization. No patient included in the study was referred to the vascular surgery department to undergo emergency coronary artery bypass grafting (CABG) surgery. Before the intervention, patients were given 300 mg of aspirin and 300 mg of clopidogrel or 180 mg of ticagrelor and low-molecular-weight heparin as per guidelines. CBCs were performed in all patients within two hours of their emergency admission. From the haemogram parameters, white blood cells (WBC), haemoglobin (Hb), platelets (Plt), mean platelet volume (MPV), neutrophils, lymphocytes, and IG values were recorded. From the biochemical parameters, high-sensitive troponin-T (hsTnT), C-reactive protein (CRP), creatinine, and glucose levels measured in the emergency room and high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, total cholesterol, and triglyceride levels measured within 24 hours after hospital admission were recorded. The IG count, as a routine parameter in CBC, was measured using a Sysmex XN-1000 modular system (Sysmex, Kobe, Japan). In-hospital mortality rates were examined. Left ventricular ejection fraction (LVEF) was recorded based on echocardiography reports. Killip classification system classes recorded at the time of admission were recorded and accepted as baseline characteristics. Patients were divided into two groups as patients with low (<0.6) and high (≥0.6) IG counts and compared.
Statistical Analysis
Statistical analyses were performed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean±standard deviation and categorical variables were expressed as numbers (n) and percentages (%). Categorical data were analysed using the chi-square test. Regarding the conformity of data to a normal distribution, the independent t-test or the Mann-Whitney U test was used, when appropriate. The optimum cut-off value of the IG count in predicting in-hospital mortality in patients with STEMI was evaluated by the receiver operating characteristic (ROC) analysis. Variables that could act on mortality were evaluated by logistic regression analysis. A P-value of <0.05 was considered statistically significant.
RESULTS
A total of 146 patients who met the inclusion criteria were included in the study. Of these patients, 112 (76.7%) were men and 34 (33.3) were women. The mean age of the patients was 62.65±14.06 years. Mean ejection fraction (EF) was 44% (30-52%), mean systolic blood pressure (SBP) was 140 (80-160), and mean diastolic blood pressure (DBP) was 85 (60-95). Seventy-four (50.7) patients met the class I criteria according to the Killip classification. The most common myocardial infarction (MI) types were inferior (46.6%) and anterior (44.5%) MI in decreasing order of frequency. Hypertension, dyslipidaemia and diabetes were the most common risk factors. The mean WBC count was 11.98±4.89. The mean CRP and IG values were 35.16±18.75 and 0.61±0.51, respectively. Table 1 presents the baseline clinical characteristics of patients with STEMI. When patients were divided into groups according to in-hospital mortality, 123 (84.2%) were in the survivor group and 23 (15.8%) were in the non-survivor group. The mean age of patients was found to be significantly higher in the non-survivor group (74.86±13.14 vs. 60.36±13.06, P<0.001). The number of male patients was significantly higher in the survivor group (P=0.002). Mean SBP, DBP, heart rate (HR) values and the percentage of patients in Killip class I were significantly higher in the survivor group compared to the non-survivor group (P<0.05 for all markers). Mean WBC, neutrophils, glucose, blood urea nitrogen (BUN), creatinine, alanine transaminase (ALT) and troponin levels were significantly higher but the mean haemoglobin levels were significantly lower in non-survivors compared to survivors (P<0.05 for all markers). Mean IG counts were significantly higher in non-survivors compared to survivors (1.12±0.22 vs. 0.50±0.28, P<0.001). The comparison of demographic data and laboratory values between groups are presented in Table 1.
| Variables | Survivors (n=123) | Non-survivors (n=23) | P-value |
|---|---|---|---|
| Age (years) | 60.36±13.06 | 74.86±13.14 | <0.001 |
| Male gender, n(%) | 100 (81.3) | 12 (52.2) | 0.002 |
| SBP, mmHg | 146 (85-172) | 110 (70-140) | <0.001 |
| DBP, mmHg | 90 (70-110) | 72 (62-82) | 0.003 |
| Heart rate, beats/min | 82.58±18.73 | 85.47±25.28 | 0.411 |
| Ejection fraction, % | 45 (40-60) | 35 (30-54) | <0.001 |
| Killip class | <0.001 | ||
| I | 73 (59.3) | 1 (4.3) | |
| II | 34 (27.6) | 2 (8.7) | |
| III | 15 (12.2) | 12 (52.2) | |
| IV | 1 (0.9) | 8 (34.8) | |
| Type of MI | 0.389 | ||
| Anterior MI | 55 (44.7) | 10 (43.5) | |
| Inferior MI | 55 (44.7) | 13(56.5) | |
| Posterior and RV MI | 9 (7.3) | 0 (0) | |
| High lateral MI | 4 (3.3) | 0 (0) | |
| Previous history | |||
| Hypertension | 64 (52.0) | 15 (65.2) | 0.244 |
| Diabetes mellitus | 39 (31.7) | 10 (43.5) | 0.273 |
| Dyslipidemia | 44 (35.8) | 11 (47.8) | 0.274 |
| History of CAD | 38 (30.9) | 6 (26.1) | 0.645 |
| Laboratory findings | |||
| WBC count (×103/mm3) | 11.42±4.15 | 14.96±7.15 | 0.021 |
| Neutrophils (×103/mm3) | 7.73±3.61 | 11.33±6.91 | <0.001 |
| Lymphocytes (×103/mm3) | 2.61±1.74 | 2.65±2.11 | 0.777 |
| Hemoglobin (mg/dL) | 14 (12-15) | 12 (9-14) | <0.001 |
| Glucose (mg/dL) | 162.08±92.86 | 232.47±28.05 | <0.001 |
| BUN | 19.10±10.17 | 30.91±4.22 | 0.002 |
| Creatinine (mg/dL) | 1.1 (0.5-1.2) | 1.2 (0.7-1.3) | <0.001 |
| Alanine transaminase (IU/L) | 28.31±19.86 | 93.43±37.58 | 0.027 |
| IG% | 0.50±0.28 | 1.12±0.22 | <0.001 |
| CRP (mg/dL) | 21.22±7.48 | 37.62±22.04 | 0.327 |
| Troponin T (ng/L) | 644.71±148.75 | 1610±448.15 | 0.003 |
| Lipid profiles (mg/dL) | |||
| Triglycerides | 120.61±95.58 | 160.21±29.56 | 0.131 |
| Total cholesterol | 204.95±53.33 | 193.86±63.83 | 0.273 |
| High-density lipoprotein | 44.43±10.98 | 42.65±12.49 | 0.509 |
| Low-density lipoprotein | 140.63±57.22 | 117.17±42.69 | 0.118 |
BUN=blood urea nitrogen; CRP=C-reactive protein; DBP=diastolic blood pressure; IG=immature granulocytes; MI=myocardial infarction; RV=right ventricular; SBP=systolic blood pressure; WBC=white blood cells

When patients were divided into two groups as those with low (<0.6) and high (≥0.6) IG counts, it was observed that there were 94 (64.3%) and 52 (35.7%) patients in the low and high IG groups, respectively. Patients with high IG counts had significantly lower SBP and DBP values. Laboratory analysis results showed that patients in the high IG count group had significantly higher WBC (14.41±6.38 vs. 10.63±3.14, P<0.001), neutrophil (10.23±5.99 vs. 7.23±2.84, P<0.001), glucose (193.41±94.95 vs. 161.97±94.99, P=0.009), BUN (23.50±13.79 vs. 19.56±12.55, P=0.03) and creatinine (1.34±0.71 vs. 1.11±0.54, P=0.001) levels compared to the low IG count group. Furthermore, mortality rates were significantly higher in the high IG count group compared to the low IG count group (26.9% vs. 9.6%, P=0.006) (Table 2).
| Variables | Low-IG group (<0.6, n=94) | High-IG group (≥0.6, n=52) | P-value |
|---|---|---|---|
| Age (years) | 62.54±13.63 | 63.00±14.96 | 0.997 |
| Male gender, n(%) | 73 (77.7) | 39 (75) | 0.564 |
| SBP, mmHg | 147 (130-155) | 128 (120-136) | 0.001 |
| DBP, mmHg | 90 (80-112) | 79 (69-88) | <0.001 |
| Heart rate, beats/min | 83 (80-114) | 82 (72-96) | 0.811 |
| Ejection fraction, % | 44 (40-60) | 41 (40-55) | 0.181 |
| Killip class | 0.052 | ||
| I | 50 (53.2) | 24 (46.2) | |
| II | 27 (28.7) | 9 (17.3) | |
| III | 14 (14.9) | 13 (25) | |
| IV | 3 (3.2) | 6 (11.5) | |
| Type of MI | 0.071 | ||
| Anterior MI | 46 (48.9) | 19 (36.5) | |
| Inferior MI | 37 (39.4) | 31 (59.6) | |
| Posterior and RV MI | 7 (7.4) | 2 (3.9) | |
| High lateral MI | 4 (4.3) | 0 (0) | |
| Previous history | |||
| Hypertension | 52 (55.3) | 27 (51.9) | 0.693 |
| Diabetes mellitus | 31 (33.0) | 18 (34.6) | 0.491 |
| Dyslipidemia | 34 (36.2) | 21 (40.4) | 0.615 |
| History of CAD | 26 (27.7) | 18 (34.6) | 0.380 |
| Laboratory findings | |||
| WBC count (×103/mm3) | 10.63±3.14 | 14.41±6.38 | <0.001 |
| Neutrophils (×103/mm3) | 7.23±2.84 | 10.23±5.99 | <0.001 |
| Lymphocytes (×103/mm3) | 2.43±1.49 | 2.97±2.23 | 0.223 |
| Hemoglobin (mg/dL) | 13 (12-15) | 13 (12.5-15) | 0.134 |
| Glucose (mg/dL) | 161.97±94.99 | 193.41±94.95 | 0.009 |
| BUN | 19.56±12.55 | 23.50±13.79 | 0.030 |
| Creatinine (mg/dL) | 1.11±0.54 | 1.34±0.71 | 0.001 |
| Alanine transaminase (IU/L) | 29.31±20.38 | 55.28±17.19 | 0.365 |
| CRP (mg/dL) | 43.67±28.61 | 19.05±3.87 | 0.324 |
| Troponin T (ng/L) | 616.93±120.61 | 1117.15±352.10 | 0.739 |
| Lipid profiles (mg/dL) | |||
| Triglycerides | 116.46±73.31 | 145.61±19.98 | 0.400 |
| Total cholesterol | 201.53±52.32 | 206.25±60.01 | 0.859 |
| High-density lipoprotein | 43.41±9.69 | 45.51±13.51 | 0.545 |
| Low-density lipoprotein | 133.11±45.82 | 143.84±70.16 | 0.710 |
| Mortality | 9 (9.6) | 14 (26.9) | 0.006 |
BUN=blood urea nitrogen; CRP=C-reactive protein; DBP=diastolic blood pressure; IG=immature granulocytes; MI=myocardial infarction; RV=right ventricular; SBP=systolic blood pressure; WBC=white blood cells

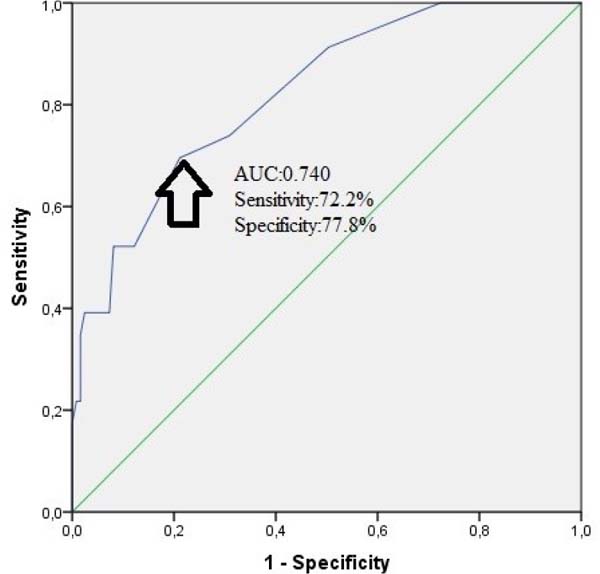
The multivariate logistic regression analysis revealed that age (OR: 7.486, 95% CI: 1.995-28.081, P=0.003), anaemia (OR: 1.634, 95% CI: 1.167-2.405, P=0.016), LVEF (OR: 0.385, 95% CI: 0.270-0.825, P=0.017), Killip class (OR: 6.382, 95% CI: 2.091-14.505, P=0.017), and IG count (OR: 5.003, 95% CI: 1.426-7.557, P<0.001) were the independent predictors of in-hospital mortality (Table 3). Furthermore, in ROC curve analysis, the IG count was shown to predict in-hospital mortality with a sensitivity of 72.2% and specificity of 77.8% at a cut-off value of 0.65 (area under the curve: 0.740, 95% CI: 0.635-0.846, P<0.001, Figure 1).
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | P | OR (95% CI) | P-value |
| Age | 7.200 (2.496-20.789) | <0.001 | 7.486 (1.995-28.081) | 0.003 |
| Male sex | 0.251 (0.098-0.639) | 0.004 | 0.455 (0.129-1.610) | 0.222 |
| LVEF (%) | 0.321 (0.232-0.550) | 0.003 | 0.385 (0.270-0.825) | 0.017 |
| Anemia | 1.233 (1.128-2.124) | 0.033 | 1.634 (1.167-2.405) | 0.016 |
| Killip class >1 | 8.211 (4.194-16.050) | 0.001 | 6.382 (2.091-14.505) | 0.017 |
| IG (%) | 3.480 (1.386-8.736) | <0.001 | 5.003 (1.426-7.557) | 0.012 |
CRP=C-reactive protein; IG=immature granulocytes; LVEF=left ventricular ejection fraction

DISCUSSION
Early assessment and treatment are of great importance in patients with cardiovascular disease associated with high mortality, such as STEMI[11]. In previous studies, several biomarkers, including troponin, CRP, N-terminal pro-brain natriuretic peptide (NT-proBNP) and NLR, as well as clinical scoring, were used as prognostic indicators. A haemogram, which is a simple test that can be easily evaluated by all physicians, is requested in almost all patients who are admitted to an emergency department or intensive care unit. The IG count is less known among physicians, but it is a simple haemogram parameter. Several studies have recently suggested that the IG count can be used to predict both the short- and long-term mortality associated with many diseases[12,13]. The present study has shown that the IG count is an independent risk factor that can be used to predict the prognosis in patients with STEMI.
The association between MI and inflammation has been known for many years. Furthermore, inflammation is closely associated with the prognosis and possible complications in patients with STEMI[14]. Increasing intensity of inflammation increases the likelihood that atherosclerotic plaques can lead to MI[15]. In many previous studies, haemogram parameters (e.g. WBC, neutrophil counts, etc.) and the ratios of such parameters to each other have been reported to have a prognostic value in patients with coronary artery disease and STEMI[16-19]. The present study has shown an association between the IG count, a simple haemogram parameter, and poor prognosis in STEMI patients.
The IG count shows the number of serial myelocytic cells in the peripheral blood and can be obtained by means of automated blood cell analysers[20]. Inflammation and trauma are known to lead to the occurrence of circulating immature cells that normally should not be present in the peripheral blood. Therefore, the diagnostic and prognostic values of circulating immature cells in sepsis, trauma, and gastrointestinal system diseases have been discussed in many studies[12,20,21]. Krishnan et al.[22] reported that the IG count was an effective marker in predicting the severity of the infection and determining the need for early intervention in critically ill patients. In another recent study that we have performed recently, we have reported that the IG count was associated with mortality in upper gastrointestinal system diseases and that the IG count helped predict mortality with 66.7% sensitivity and 75.7% specificity at a cut-off value of 0.95[7].
Park et al.[23] studied the diagnostic value of the IG count and its role in estimating the occurrence of complications in patients with acute appendicitis. In that study, it was shown that the IG count was not as effective as other inflammatory markers in making the diagnosis and estimating the occurrence of complications. Sinaga et al.[13] have reported that the IG count obtained at the time of admission to the emergency department serves as a marker, which could effectively help predict the 30-day mortality with a cut-off value of 1.05 in patients with peritonitis. Huang et al.[24] reported that the IG count could be a predictor of possible lung complications at the onset of acute pancreatitis. In another recent study, haematological biomarker levels measured at the time of admission of patients with acute MI were investigated as predictors of all-cause mortality. This study found that an IG count >0.3 was significantly correlated with mortality[25]. Similarly, in the present study, we have observed a significant association between high IG values and mortality in patients with STEMI. Our study results show that the IG count helps to predict in hospital mortality with 72.2% sensitivity and 77.8% specificity at a cut-off value of 0.65.
Limitations
This study has several limitations. First, it was designed as a single-centre, retrospective study. Second, the time elapsed from the onset of symptoms to the time of sampling and the time from diagnosis of STEMI to pPCI were not analysed, which might have affected our results. Lastly, serial IG counts could not be performed, and IG counts could not be compared with the levels of some inflammatory parameters such as tumour necrosis factor and interleukin 6. There is a need for prospective multi-centre studies to show that the IG count can be used as a prognostic marker in patients with STEMI.
REFERENCES
1. 1 Omer MA, Tyler JM, Henry TD, Garberich R, Sharkey SW, Schmidt CW,et al. Clinical characteristics and outcomes of STEMI patients with cardiogenicshock and cardiac arrest. JACC Cardiovasc Interv. 2020;13(10):1211-9.doi:10.1016/j.jcin.2020.04.004.
2. 2 Cui Y, Hao K, Takahashi J, Miyata S, Shindo T, Nishimiya K, et al.Age-specific trends in the incidence and in-hospital mortality of acutemyocardial infarction over 30 years in Japan - report from the Miyagi AMIregistry study. Circ J. 2017;81(4):520-8.doi:10.1253/circj.CJ-16-0799.
3 Kong T, Kim TH, Park YS, Chung SP, Lee HS, Hong JH, et al. Usefulness of the delta neutrophil index to predict 30-day mortality in patients with ST segment elevation myocardial infarction. Sci Rep. 2017;7(1):15718. doi:10.1038/s41598-017- 15878-5.
4. Bouleti C, Mewton N, Germain S. The no-reflow phenomenon: state of the art. Arch Cardiovasc Dis. 2015;108(12):661-74. doi:10.1016/j.acvd.2015.09.006.
5. Cui H, Zhang X, Ding X, Zhou L, Liang S, Qiu H, et al. Urinary alpha1-microglobulin: a new predictor for in-hospital mortality in patients with ST-segment elevation myocardial infarction. Med Sci Monit. 2021;27:e927958. doi:10.12659/ MSM.927958.
6. Tanik VO, Cinar T, Arugaslan E, Karabag Y, Hayiroglu MI, Cagdas M, et al. The predictive value of PRECISE-DAPT score for in-hospital mortality in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Angiology. 2019;70(5):440-7. doi:10.1177/0003319718807057.
7. Bedel C, Korkut M, Avcı A, Uzun A. Immature granulocyte count and percentage as new predictors of mortality in patients with upper gastrointestinal bleeding. Indian J Crit Care Med. 2020;24(9):794-8. doi:10.5005/jp-journals-10071-23563.
8. Bedel C, Korkut M, Aksoy F, Kuş G. Usefulness of immature granulocytes to predict high coronary SYNTAX score in acute coronary syndrome; a cross-sectional study. Arch Acad Emerg Med. 2020;8(1):e73.
9. Korkut M, Bedel C, Selvi F. Are immature granulocytes and derivatives early predictors of acute appendicitis and acute complicated appendicitis in adults? Formos J Surg. 2020;53(4):123-7. doi:10.4103/ fjs.fjs_111_19.
10. O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll Cardiol. 2013;61(4):e78-e140. doi:10.1016/j.jacc.2012.11.019.
11. Çağdaş M, Karakoyun S, Yesin M, Rencüzoğulları İ, Karabağ Y, Uluganyan M, et al. The association between monocyte HDL-C ratio and SYNTAX score and SYNTAX score II in STEMI patients treated with primary PCI. Acta Cardiol Sin. 2018;34(1):23-30. doi:10.6515/ ACS.201801_34(1).20170823A.
12. Bedel C, Korkut M, Selvi F, Zortuk Ö. The immature granulocyte count is a new predictor of the 30-day mortality in intracerebral haemorrhage patients: preliminary study. Indian J Neurosurg. 2021;10(2):114-20. doi:10.1055/s-0040-1721627.
13. Sinaga RH, Utariani A, Wardhani P, Hardiono H. Immature granulocyte and mean platelet volume as a predictor of 30-day postoperative mortality in patients with sepsis caused by peritonitis. Bali J Anesthesiol. 2020;4(4):166-71. doi:10.4103/BJOA.BJOA_114_20.
14. Gul I, Cerit L, Senturk B, Alkan MB, Kemal H, Cerit Z, et al. The importance of intra-aortic pulse pressure after anterior ST-segment elevation myocardial infarction. Braz J Cardiovasc Surg. 2018;33(6):579-87. doi:10.21470/1678-9741-2018-0106.
15. Mozos I, Malainer C, Horbańczuk J, Gug C, Stoian D, Luca CT, et al. Inflammatory markers for arterial stiffness in cardiovascular diseases. Front Immunol. 2017;8:1058. doi:10.3389/fimmu.2017.01058.
16. Klein A, Wiberg S, Hassager C, Winther-Jensen M, Frikke-Schmidt R, Bang LE, et al. Admission leukocyte count is associated with late cardiogenic shock development and all-cause 30-day mortality in patients with st-elevation myocardial infarction. Shock. 2020;53(3):299-306. doi:10.1097/SHK.0000000000001369.
17. Gurbuz O, Kumtepe G, Ozkan H, Karal IH, Velioglu Y, Ercan A, et al. Predictive value of neutrophil-lymphocyte ratio for long-term cardiovascular event following coronary artery bypass grafting. Braz J Cardiovasc Surg. 2020;35(3):274-84. doi:10.21470/1678-9741- 2018-0362.
18. Esenboğa K, Kurtul A, Yamantürk YY, Tan TS, Tutar DE. Systemic immune-inflammation index predicts no-reflow phenomenon after primary percutaneous coronary intervention. Acta Cardiol. 2021:1-8. doi:10.1080/00015385.2021.1884786.
19. Kurtul A, Ornek E. Platelet to lymphocyte ratio in cardiovascular diseases: a systematic review. Angiology. 2019;70(9):802-18. doi:10.1177/0003319719845186.
20. Lima LR, Cunha GS, Nogueira KS, Comar SR. Automated immature granulocyte count in patients of the intensive care unit with suspected infection. J. Bras. Patol. Med. Lab. 2019;55(3):267-80. doi:10.5935/1676-2444.20190031.
1. Jayasekara WM, Kulathilake C, Wijesekara S, Wijesiriwardena I. Role of manual immature to total neutrophil (I/T) ratio and automated immature granulocyte count (IGC) and Percentage (IG%) in the early diagnosis of neonatal sepsis. Res Sq 2021 Jan 29:1- 23. doi:10.21203/rs.3.rs-154297/v1.
22. Krishnan H, Yogalakshmi E, Chander V, Muthuvel E. Clinical utility of immature granulocyte percentage and NLR in Critical care unit patients in a tertiary care hospital. Ann Trop Med Health. 2020;23:2323-100.
23. Park JS, Kim JS, Kim YJ, Kim WY. Utility of the immature granulocyte percentage for diagnosing acute appendicitis among clinically suspected appendicitis in adult. J Clin Lab Anal. 2018;32(7):e22458. doi:10.1002/jcla.22458.
24. Huang Y, Xiao J, Cai T, Yang L, Shi F, Wang Y, et al. Immature granulocytes: a novel biomarker of acute respiratory distress syndrome in patients with acute pancreatitis. J Crit Care. 2019;50:303-8. doi:10.1016/j.jcrc.2018.12.002.
25. Monteiro Júnior JGM, Torres DOC, da Silva MCFC, Martins CMH, da Silva IK, do Nascimento MEM, et al. Prognostic value of hematological parameters in patients with acute myocardial infarction: intrahospital outcomes. PLoS One. 2018;13(4):e0194897. doi:10.1371/journal.pone.0194897.
Authors’ Roles & Responsibilities
MK = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; drafting the work or revisingit critically for important intellectual content; final approval ofthe version to be published
CB = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; drafting the work or revisingit critically for important intellectual content; final approval ofthe version to be published
RS = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; final approval of the versionto be published
MAA = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; final approval of the versionto be published
FS = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; final approval of the versionto be published
GK = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; final approval of the versionto be published
ÖZ = Substantial contributions to theconception or design of the work; or the acquisition, analysis, orinterpretation of data for the work; final approval of the versionto be published
Article receive on Tuesday, February 9, 2021
Article accepted on Monday, August 30, 2021
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket