![]()
![]()
İsmail SelçukI; Hüseyin SicimII; Ümmühan Nehir SelçukIII; Bülent Barış GüvenIV; Ahmet Turan YılmazI
DOI: 10.21470/1678-9741-2021-0439
ABSTRACT
Introduction: In this study, we aimed to present three different methods for symptomatic aberrant right subclavian artery (ARSA) surgery.AsScBp= Ascending aorta-subclavian artery bypass
CoE= Compression of esophagus
CoET= Compression of esophagus and trachea
CScBp= Carotid-subclavian artery bypass
CTA= Computed tomography angiography
DM= Diabetes mellitus
HL= Hyperlipidemia
HT= Hypertension
KD= Kommerell’s diverticulum
LMPLT= Left mini posterolateral thoracotomy
TEVAR= Thoracic endovascular aortic repair
TOAR= Thoracic open aortic repair
UMS= Upper mini sternotomy
INTRODUCTION
Aberrant right subclavian artery (ARSA) is a rare anatomical variation of the origin of the right subclavian artery, and it occurs in about 0.7% of the general population[1]. It is thought to occur in embryonic life due to the insufficiency of the inhibition mechanism during the development of the aortic arch. Most of the patients are asymptomatic throughout their lives, and the diagnosis of ARSA is made incidentally by imaging methods in most of them. As a result of the compression of the aberrant artery on the surrounding tissues, symptoms such as dysphagia, cough, and stridor may occur[2]. Dysphagia lusoria is an abnormal condition characterized by difficulty in swallowing caused by an ARSA. It was discovered by David Bayford in 1761 and first reported in a paper by him in 1787[3]. ARSA may also be associated with Kommerell’s diverticulum (KD). This diverticulum is defined as the dilation of the proximal part of the aberrant subclavian artery near its exit from the aorta and represents the embryonic residue of the dorsal aorta[4]. Aneurysmal degeneration of KD and ARSA may result in a significant risk for dissection and rupture with high mortality[5]. While ARSA treatment has traditionally been performed with open surgery to relieve symptoms or prevent complications, in recent years, treatment strategies have shifted to more hybrid or endovascular approaches[6]. Treatment is indicated for relief of symptoms and prevention of serious complications from aneurysmal dilatation.
Open vascular surgical procedures are associated with high mortality and morbidity rates, especially in elderly patients who develop symptoms and aneurysm, and are associated with a high risk of neurological events[7]. In addition to open vascular surgery methods, endovascular and combined hybrid methods are applied as different techniques in order to reduce the complications that may develop postoperatively and to obtain better results[8].
With this study, we aimed to contribute to the determination of the most accurate strategy in terms of results by presenting three different surgical treatment strategies in patients with ARSA and/or aneurysm.
METHODS
Between January 2016 and December 2020, symptomatic ARSA was diagnosed in 11 patients. The data of all patients were analyzed retrospectively. Demographic data, current medical conditions, symptoms, radiological images, treatment techniques, and postoperative results of the patients were recorded (Table 1). In all patients, the location of the aberrant artery was confirmed by contrast-enhanced tomography for the analysis of anatomical structures. All patients were evaluated with computed tomography angiography (CTA).
| Patient (sex/age) |
Comorbidities | Pathology | Symptoms | Supra-aortic correction | Aortic approach | Complications | Outcomes |
|---|---|---|---|---|---|---|---|
| 1) Male (57) | None | Aneurysmatic ARSA with CoET | Dysphagia + dyspnea | Bilateral CScBp | TEVAR | Continuing dysphagia cause of persisting esophageal compression | Partial symptom relief after esophageal dilatation |
| 2) Female (53) | None | Aneurysmatic ARSA with CoE | Dysphagia | Bilateral CScBp | TEVAR | Continuing dysphagia cause of persisting esophageal compression | Patient disapproved additional procedure |
| 3) Male (62) | DM, HT | Aneurysmatic ARSA with CoE | Dysphagia | Bilateral CScBp | TEVAR | None | Symptom free |
| 4) Female (51) | None | ARSA | Dysphagia | Bilateral CScBp | TEVAR | None | Symptom free |
| 5) Male (52) | None | Aneurysmatic ARSA with CoE | Dysphagia | Right CScBp | TOAR (LMPLT) | Plexus brachialis injury | Right upper extremity weakness |
| 6) Female (53) | DM, HL | ARSA with CoE | Dysphagia | Right CScBp | TOAR (LMPLT) | None | Symptom free |
| 7) Male (61) | Smoker | ARSA | Dysphagia | Right CScBp | TOAR (LMPLT) | None | Symptom free |
| 8) Female (54) | None | Aneurysmatic ARSA with CoET | Dysphagia + dyspnea | AsScBp | TOAR (UMS + LMPLT) | Right pleural effusion (treated with thoracentesis) | Symptom free |
| 9) Female (58) | Smoker | Aneurysmatic ARSA with CoET | Dysphagia + dyspnea | AsScBp | TOAR (UMS + LMPLT) | Recurrent laryngeal nerve paralysis | Soft hoarseness |
| 10) Female (55) | HL, HT | ARSA with CoE | Dysphagia | AsScBp | TOAR (UMS + LMPLT) | None | Symptom free |
| 11) Female (49) | None | ARSA | Dysphagia | AsScBp | TOAR (UMS + LMPLT) | None | Symptom free |
ARSA=aberrant right subclavian artery; AsScBp=ascending aorta-subclavian artery bypass; CoE=compression of esophagus; CoET=compression of esophagus and trachea; CScBp=carotid-subclavian artery bypass; DM=diabetes mellitus; HL=hyperlipidemia; HT=hypertension; LMPLT=left mini posterolateral thoracotomy; TEVAR=thoracic endovascular aortic repair; TOAR=thoracic open aortic repair; UMS=upper mini sternotomy

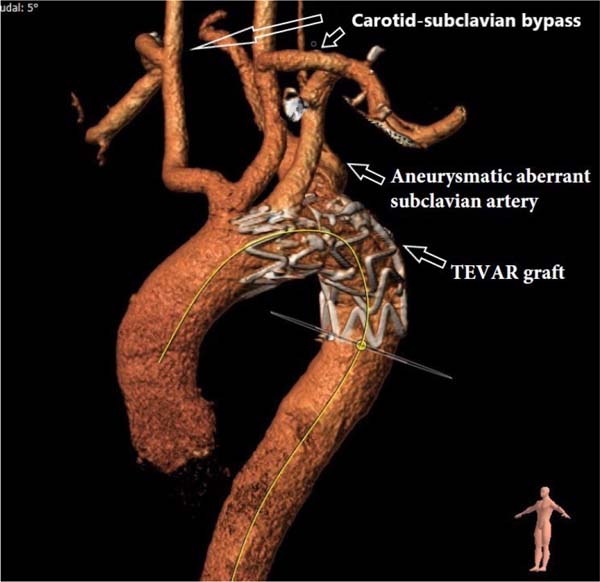
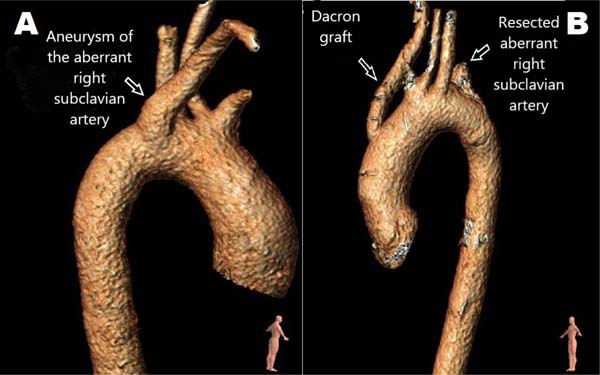
Dysphagia symptom was present in all our patients as an indication for surgical correction; in addition, three of our patients had dyspnea. Aneurysm was present in six patients; one of the aneurysmatic ARSAs required emergency surgical intervention due to dissection. Hybrid procedure was applied to the first four patients by performing bilateral carotid-subclavian artery bypass (CScBp) and thoracic endovascular aortic repair (TEVAR) (Figure 1). In the first session, patients underwent bilateral CScBp operation. In the second session, TEVAR procedure was applied to the patients, and ARSA occlusion was achieved. In the second group of patients, both right CscBp operation and thoracic open aortic repair (TOAR) were performed in the same session (Figure 2). In the third group of patients, aortic graft operation was performed from the ascending aorta to the right carotid bypass and TOAR in the same session (Figure 3).




RESULTS
Median age of the 11 patients (7 females/4 males) was 55 years (range 49 - 62). The treatment was performed with open surgery in seven patients (63.7%) and hybrid approach in four patients (36.3%). The demographic data of the patient groups who underwent three different approaches were analyzed, and no significant difference was found between them. ARSA was passing from the dorsal mediastinum to the esophagus in all 11 patients. All patients were symptomatic (dysphagia n=8 and dysphagia + dyspnea n=3). ARSA itself had aneurysmal dilatation in six patients (50%).
No patient had ruptured KD, but one had dissection of the ARSA (patient #5). Due to the sudden onset of symptoms, this patient underwent emergency operation. All other patients underwent elective surgery. Aneurysmatic ARSA was present in three of four patients who underwent bilateral CScBp + TEVAR. Four patients had dysphagia; one patient had dyspnea in addition to dysphagia. As a result of the two-stage operation, persisting esophageal compression was observed in two (50%) patients. Esophageal dilatation was applied to these patients, and symptoms were relieved. No endoleak was detected in the control CTA examinations performed in these patients who underwent the hybrid procedure.
All three patients who underwent right CScBp + TOAR had dysphagia. One patient in this patient group underwent emergency surgery due to dissection. No complications developed, and relief was observed in symptoms. Brachial plexus injury developed in one of the patients in this group. Right upper extremity weakness was observed in the postoperative period.
Of the four patients who underwent ascending aorta-subclavian artery bypass (AsScBp) + TOAR operation, four had dyspnea and two had dysphagia + dyspnea. These patients underwent elective anatomic bypass from the ascending aorta to the right subclavian artery and TOAR. In the postoperative period, pleural effusion developed in one patient, and relief was achieved only with thoracentesis. Hoarseness due to recurrent laryngeal nerve paralysis developed in one patient, and full recovery was observed with medical treatment at the three-month follow-up.
DISCUSSION
ARSA is the most common anomaly involving the aortic arch with an incidence of 0.5 to 2.5%[9]. It originates after the left subclavian artery as the last branch of the aortic arch, turns from the back, and passes to the right. Although rare, it sometimes passes between the esophagus and the trachea or in front of the trachea. It is known that most of ARSA patients are asymptomatic. Symptomatic patients may present with different complaints. Dysphagia, dyspnea, or pneumonia complaints may occur due to esophageal or tracheal compression[10]. Symptoms may become more pronounced and worsen with advancing age. Although rare, complications such as aneurysmal dilatation, right arm ischemia, rupture, and fistulization can be seen[11].
In the diagnostic sense, CTA and magnetic resonance angiography examinations are very important in revealing the anatomy of the anomaly and in the treatment strategy. Awareness of this anomaly is of clinical importance, as it may be associated with tracheoesophageal compression symptoms, aneurysm formation, or aneurysm rupture. It causes the appearance of an upper mediastina mass in both lesions. Recognition of ARSA is surgically important. In these cases, it is necessary to know the recurrent nerve tracing well. In addition, inadvertent placement of the cross-clamp proximal to the left subclavian artery during surgery may cause serious cerebral pathologies.
The first successful surgical treatment of ARSA was described by Gross in 1946[12]. In 1965, Bailey et al.[12] reanastomosed ARSA from the right thoracotomy to the ascending aorta. Orvald et al.[13] anastomosed the right subclavian artery to the right common carotid artery with only a cervical incision. Hybrid methods can also be applied in symptomatic ARSA patients in the light of developing technology and current approaches. We also used the hybrid approach in the first four patients in our published series. However, there was no regression in dysphagia complaints due to postoperative compression findings. Whereas, Vucemilo et al.[14] reported that although no shrinkage in the aneurysm was observed in patients with hybrid treatment, symptomatic ARSA and compression findings were reduced. The low number of cases is thought provoking as to whether TEVAR has any symptom-relieving effect. Morris et al.[15] used an Amplatzer Vascular Plug (St. Jude Medical, Saint Paul, Minnesota, United States of America) to occlude the proximal part of the abnormal right subclavian artery in a hybrid study. They then performed a CScBp via a supraclavicular incision. In such hybrid methods, dysphagia may be permanent or may be a risk factor for arterioesophageal fistula.
Apart from hybrid methods, there are also studies on open surgical applications. Van Son et al.[16] surgically approached the mobilization of ARSA through a right thoracotomy, separating the vessel at its origin without leaving a long stump. Since the results of the hybrid method were not satisfactory in our clinical series, surgical repair methods were used. We performed CScBp + TOAR on three of our patients after our hybrid method applications. Among the postoperative results of the surgical technique we applied, we observed brachial plexus injury in one of these three patients. Despite the medical treatment, the postoperative long-term complication continued. In order to reduce the complication rates, we switched to the AsScBp + TOAR operation strategy, which is an anatomical bypass, in subsequent cases. Recurrent laryngeal nerve paralysis complication was observed in one of these four patients in the postoperative period. As a result, the patient developed hoarseness. Keiffer et al.[17] emphasized the anatomical variations associated with ARSA in their study. These include abnormal origin of the right vertebral artery from the aorta or right common carotid artery, presence of a common carotid trunk, right-sided thoracic duct, and a non-recurrent laryngeal nerve.
When the laryngeal nerve is not recurrent, it originates from the vagus nerve in the neck and directly innervates the larynx. Although this anomaly is less important than others for the surgical treatment of ARSA, it is important to recognize it in patients who may require a carotid artery or thyroid procedure. The surgeon should identify and protect the vagus and recurrent laryngeal nerves while performing vascular exploration to avoid any neurological complication in the postoperative period. In posterior mediastina exploration, dissection close to the vessel may reduce the risk of neural damage. We think that left thoracotomy reduces the risk of laryngeal nerve injury in patients without aneurysm, especially the risk of left recurrent nerve injury near the source of ARSA.
Treatment indications and timing for ARSA is also a subject of discussion. Austin and Wolfe[18] reported fatal rupture cases in 19% of the patients, and some of them showed dissection association. Therefore, many authors support fairly early interventions for these cases. In the case series that we have presented, we had to undergo an emergency operation with the development of dissection in an aneurysm in one of our patients. Complications that may occur if it is delayed may be mortal. Patient-specific characteristics, age, comorbid factors, anatomy, and potential risks of the procedure should be considered in determining the treatment strategy. Open repair may be more challenging and riskier in clinically challenging cases.
There is no standard treatment selection algorithm in current treatment methods and in this retrospective study. It is very difficult to compare hybrid or other surgical methods with each other. This work we have done can contribute to the decision-making process.
CONCLUSION
Surgical treatment of symptomatic ARSA patients is a very challenging operation. Different surgeons on this subject apply different surgical methods, and there is no common consensus. With the developing technology, hybrid methods or combined surgical strategies can be applied. However, the benefits and harms of all of them are still among the controversial issues. In this study, we also presented three different surgical approaches, one of which is hybrid, and their results.
As a result of the comparison of these three techniques that we have applied in our clinic, we think that the AsScBp + TOAR approach is more appropriate because it has anatomical bypass, less risk of complications, and more successful surgical results. More case series are needed to further clarify this issue.
REFERENCES
1. Popieluszko P, Henry BM, Sanna B, Hsieh WC, Saganiak K, Pękala PA, et al. A systematic review and meta-analysis of variations in branching patterns of the adult aortic arch. J Vasc Surg. 2018;68(1):298-306.e10. doi:10.1016/j.jvs.2017.06.097.
2. Knight GC, Codd JE. Anomalous right subclavian artery aneurysms. Report of 3 cases, with a review of the literature. Tex Heart Inst J. 1991;18(3):209-18.
3. Asherson N. David Bayford. His syndrome and sign of dysphagia lusoria. Ann R Coll Surg Engl. 1979;61(1):63-7.
4. Hogg JP, Dominic AJ, Counselman RL, Hurst JL. Expanding aneurysm of aberrant right subclavian artery. Case report and imaging evaluation. Clin Imaging. 1997;21(3):195-9. doi:10.1016/s0899-7071(96)00026-5.
5. Austin EH, Wolfe WG. Aneurysm of aberrant subclavian artery with a review of the literature. J Vasc Surg. 1985;2(4):571-7. doi:10.1067/mva.1985.avs0020571.
6. van Bogerijen GH, Patel HJ, Eliason JL, Criado E, Williams DM, Knepper J, et al. Evolution in the management of aberrant subclavian arteries and related kommerell diverticulum. Ann Thorac Surg. 2015;100(1):47-53. doi:10.1016/j.athoracsur.2015.02.027. [MedLine]
7. Stone WM, Ricotta JJ 2nd, Fowl RJ, Garg N, Bower TC, Money SR. Contemporary management of aberrant right subclavian arteries. Ann Vasc Surg. 2011;25(4):508-14. doi:10.1016/j.avsg.2011.02.012.
8. Myers PO, Fasel JH, Kalangos A, Gailloud P. Arteria lusoria: developmental anatomy, clinical, radiological and surgical aspects. Ann Cardiol Angeiol (Paris). 2010;59(3):147-54. doi:10.1016/j.ancard.2009.07.008.
9. Gross RE, Neuhauser EB. Compression of the trachea by an anomalous innominate artery; an operation for its relief. Am J Dis Child. 1948;75(4):570-4. doi:10.1001/archpedi.1948.02030020585007.
10. Kieffer E, Bahnini A, Koskas F. Aberrant subclavian artery: surgical treatment in thirty-three adult patients. J Vasc Surg. 1994;19(1):100-9; discussion 110-1. doi:10.1016/s0741-5214(94)70125-3.
11. Gross RE. Surgical treatment for dysphagia lusoria. Ann Surg. 1946;124:532-4.
12. Bailey CP, Hirose T, Alba J. Re-establishment of the continuity of the anomalous right subclavian artery after operation for dysphagia lusoria. Angiology. 1965;16(9):509-13. doi:10.1177/000331976501600901.
13. Orvald TO, Scheerer R, Jude JR. A single cervical approach to aberrant right subclavian artery. Surgery. 1972;71(2):227-30.
14. Vucemilo I, Harlock JA, Qadura M, Guirgis M, Gowing RN, Tittley JG. Hybrid repair of symptomatic aberrant right subclavian artery and kommerell's diverticulum. Ann Vasc Surg. 2014;28(2):411-20. doi:10.1016/j.avsg.2013.04.016.
15. Morris ME, Benjamin M, Gardner GP, Nichols WK, Faizer R. The use of the amplatzer plug to treat dysphagia lusoria caused by an aberrant right subclavian artery. Ann Vasc Surg. 2010;24(3):416.e5-8. doi:10.1016/j.avsg.2009.06.027.
16. van Son JA, Mierzwa M, Mohr FW. Resection of atherosclerotic aneurysm at origin of aberrant right subclavian artery. Eur J Cardiothorac Surg. 1999;16(5):576-9. doi:10.1016/s1010-7940(99)00243-2.
17. Kieffer E, Bahnini A, Koskas F. Aberrant subclavian artery: surgical treatment in thirty-three adult patients. J Vasc Surg. 1994;19(1):100-9; discussion 110-1. doi: 10.1016/s0741-5214(94)70125-3.
18. Austin EH, Wolfe WG. Aneurysm of aberrant subclavian artery with a review of the literature. J Vasc Surg. 1985;2(4):571-7. doi: 10.1067/mva.1985.avs0020571.
Authors’Roles & Responsibilities
İS = Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
HS = Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; final approval of the version to be published
UNS = Final approval of the version to be published
BBG = Final approval of the version to be published
ATY = Drafting the work or revising it critically for important intellectual content; final approval of the version to be published
Article receive on Friday, August 20, 2021
Article accepted on Thursday, November 11, 2021
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket