![]()
![]()
Claudinei CollatussoI; João Gabriel RoderjanII; Eduardo Discher VieiraIII; Francisco Diniz Affonso da CostaIV; Lucia de NoronhaV; Daniele de Fátima FornazariVI
DOI: 10.5935/1678-9741.20120013
CO2: carbon dioxide
GDA: glutaraldehyde
GL: L-glutamic acid
HE: hematoxylin-eosin
PVPI: povidone iodine
SDS: sodium dodecyl sulfate
INTRODUCTION
The use of glutaraldehyde (GDA) as tissue fixation agent [1] made it possible for heart valve prostheses constructed with heterologous tissue could be used clinically with good results. In addition to being effective in sterilization and in reducing tissue antigenicity by masking of cellular antigens, GDA increases the biomechanical strength of the tissues which can imply better durability of bioprostheses. However, the tissue degeneration of dystrophic calcification is still problematic, especially in children and young adults [2].
The factors influencing calcification are multifactorial including the phospholipid composition of extracellular matrix, the intensity of inflammatory and immune responses to heterologous tissue and the mechanical stress caused by the movement of opening and closing the valve leaflets. Moreover, there is evidence that the proper fixing with glutaraldehyde also promotes the process of dystrophic calcification [3,4]. In an attempt to eliminate or delay this complication, several anti-calcification methods were tested, with varying degrees of success [5]. These methods aim primarily to remove the calcifying components of the tissue or neutralize the toxic effects of residual aldehydes [6-12].
It is well established that the cells and cellular debris present in the tissue constitute fixed initial outbreaks of crystallization. For they are devitalized, there is an imbalance in the calcium transport in these cells that leads to increased intracellular calcium, which binds to cell membrane phospholipids, with consequent formation of calcium phosphate crystals. Therefore, the technology of tissue decellularization allows to obtain acellular matrices that, at least in theory, are less immunogenic and with reduced potential for calcification [13-17].
Our research group at the Pontifícia Universidade Católica do Paraná (PUCPR) developed decellularization technology of homografts based on solution of sodium dodecyl sulfate (SDS). The experimental and clinical results of studies have demonstrated that aortic homograft and pulmonary homografts are less immunogenic and capable of being repopulated "in vivo" after implantation. Furthermore, there was no calcification of both cusps as in the arterial wall of the grafts, even in grafts implanted in children and adolescents up to 6 years of clinical outcome [18,19].
This study intends to verify experimentally in rats, if SDS decellularization applied to the bovine pericardium fixed in glutaraldehyde prostheses commercially available is also effective in reducing calcification in this situation.
METHODS
The bovine pericardium were obtained from local abattoirs and sent immediately to the laboratory where it was held mechanically cleaning of the fat from the the pericardial surface, cut into pieces of 10 cm2 and then stored in a phosphate buffer solution (0.1 M PBS pH 7.4 - Sigma, IL) at 4ºC. The pericardium was divided into four groups according to the method of tissue treating:
• Group 1 (GDA - Control Group) - Fresh pericardium fixed in glutaraldehyde (0.5% glutaraldehyde purified on charcoal by filtration - Merck, Germany) in phosphate buffer (PBS 0,1M pH 7,4 - Sigma, IL, USA) (v / v) for 72 hours at 20 ºC;
• Group 2 (GDA-GL) - GDA 0.5% (glutaraldehyde purified on charcoal by filtration - Merck, Germany) in phosphate buffer (PBS 0,1M pH 7,4 - Sigma, IL, USA) (v / v) for 72 hours at 20 º C and subsequently treated with 0.2% glutamic acid (Sigma, IL, USA) (m / v) in phosphate buffer (PBS 0,1M pH 3,5 - Sigma, IL) for 24 hours at 20 º C;
•Group 3(D-GDA) - pericardium decellularized in 0.1% SDS (Brazilian patent PI 800603-2) and then fixed in 0.5% glutaraldehyde (Merck, Germany) for 72 hours;
•Group 4 (D-GDA-GL) - pericardium decellularized in 0.1% SDS, and then fixed in glutaraldehyde (0.5% glutaraldehyde purified on charcoal by filtration - Merck, Germany) for 72 hours at 20 º C; subsequently treated with 0.2% glutamic acid (Sigma, IL, USA) (m / v) in phosphate buffer (PBS 0,1M pH 3,5 - Sigma, IL,USA) for 24 hours at 20 ºC.
All procedures for preparation of the pericardium were performed in a laminar flow, using sterile instruments and solutions, following the guidelines of Good Manufacturing Practices. The fragments of the groups that involved pericardium decellularization were analyzed by hematoxylineosin (HE) to confirm the complete removal of the cells (Figure 1).

Samples were prepared for implantation by cutting the four pericardium segments of each treatment group, in 18 samples of 0.5 cm2 each, which were maintained in sterile saline solution until the time of implantation in the subcutaneous tissue of rats.
Subcutaneous implantation in rats
For testing of calcification it was used the experimental model in the subcutaneous tissue of young rats [18].
All procedures were performed in accordance with the "Guide for Care and Use of Laboratory Animals" published in the U.S. National Institute Health (NIH publication 85-23, revised in 1996).
This study was approved by the Ethics Committee on Animal Use - CEUA PUC-PR, No. 620.
The study included rats of the Sprague-Dawley strain (CEMIB - Campinas, SP, Brazil), aged four weeks old, weighing between 70 and 90 g, with an implanted pericardium of each group in each animal. A total of 18 rats were used, which were anesthetized with 10 mg / g of ketamine (Crystalia, Brazil) and 3 mg / g of xylazine (Bayer, Brazil) by intraperitoneal injection. The animals were placed in the prone position, then it was performed trichotomy of the dorsal and then made asepsis with povidone-iodine (PVP - Segment, Brazil). The pericardium segments were implanted in four distinct areas: the left scapular region -GDA Group; right scapular region - GDA-GL group, the left lumbar region - D-GDA group, and right lumbar region - DGDA-GL group. After surgery, the animals received antibiotics - cefazolin sodium 4 mg / kg (ABL, Brazil) and analgesic - dipyrone 10 mg / g (Bayer, Brazil) was administered for 3 days. The animals were housed in cages with sawdust controlled and received food and water ad libitum.
The animals were divided into two groups of nine rats each, according to the time of explant. The first group included nine animals that had the pericardium explanted at 45 days and the second group involved the remaining nine rats that had the pericardium explanted at 90 postoperative days. For explants, the animals were anaesthetized with anesthetic and the same protocol, and then were euthanized in a chamber of CO2. Samples were withdrawn from the subcutaneous skin incision and removal of adhesions, and washed in isotonic saline, and cut into two equal parts. The first half was used for histomorphological analysis and another for measuring the concentration of calcium by atomic absorption spectrometry.
Atomic absorption spectrometry
The samples for atomic absorption spectrometry for quantitation of calcium, were dried at 200ºC in an oven for 2 hours, weighed in its entirety and hydrolyzed in glass tubes containing 1 ml of 6M hydrochloric acid. The tubes were heated to 92ºC water bath. After the process, the hydrolyzed samples were sent for analysis using the instrument PERKIN ELMER 4100 (LACTEC - PR, Brazil), and the results expressed in mg of calcium per mg of tissue - bovine pericardium.
Histomorphological analysis
The explants were fixed in 10% buffered formalin, mounted in paraffin and cut into microtome to 5 µm. The sections were mounted onto glass slides and stained with HE and Alizarin Red pH 4.2 and 7.0 (Sigma, IL, USA). The histomorphological study aimed primarily to evaluate the intensity and characteristics of the inflammatory infiltrate and calcification.
The histopathological characteristics of the inflammatory infiltrate were made according to the methodology described by Maizato et al.20, which include the analysis of the presence of granulomatous reaction, mononuclear infiltrate, granulomatous tissue, necrotic tissue and bacteria. Quantification was based on the percentile extension seen in the microscopic fields and graded from 0 to 4 as follows:
• 0: no change in the examined tissue;
• 1: changes present between 1-25% of the tissue area analyzed;
• 2: changes present between 26-56% of the tissue area analyzed;
• 3: changes present between 51-75% of the tissue area analyzed;
• 4: changes present between 76-100% of the tissue area analyzed analyzed.
The calcification analysis was performed by measuring morphometric calcified area compared to the non-calcified area, measured in histological sections stained with alizarinred in two pH's: pH 4.2 for calcium phosphate and pH 7.0 for calcium oxalate and other calcium salts resulting in a percentage of calcified tissue [10]. The morphometric analyses were performed on images captured by an optical microscope Olympus DX-40, coupled to a system of capturing images at a 100x magnification. The measurements were performed using the percentage comparison tool of software ImagePro Plus 6 being repeated twice by different observers in blind test. Measurement results were recorded in a spreadsheet and statistically analyzed.
Statistical Analysis
The results were expressed as mean, median, minimum values, maximum values and standard deviations. To compare the two groups in terms of quantitative variables, it was considered the non-parametric Mann-Whitney test. Comparisons between more than two groups were made using the non-parametric Kruskal-Wallis test. To compare the evaluation times within each group, we used the nonparametric Wilcoxon test. P values <0.05 were considered statistically significant. The data were organized into an Excel spreadsheet and analyzed with the software Statistica v.8.0.
RESULTS
Histomorphometric analysis
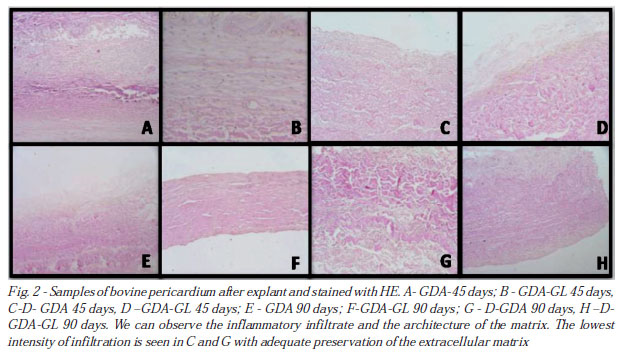
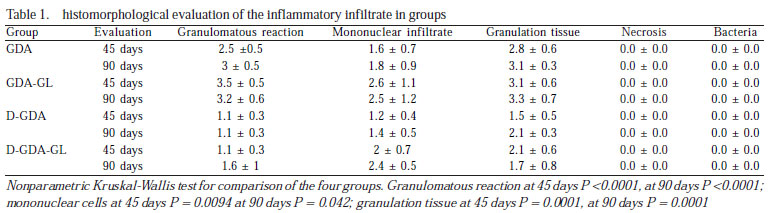
There was inflammatory infiltration with the same characteristics in the four groups (Figure 2). However, we observed that the decellularization reduced the intensity of this reaction, since the groups D-GDA and D-GDA-GL were those who had the lowest percentages of inflammatory cells, at 45 and 90 days of evolution (P <0.001 .) The pericardia from group GDA-GL presented the most pronounced inflammatory reactions when compared to other groups (Table 1). There were no areas of necrosis or the presence of bacteria in either group.
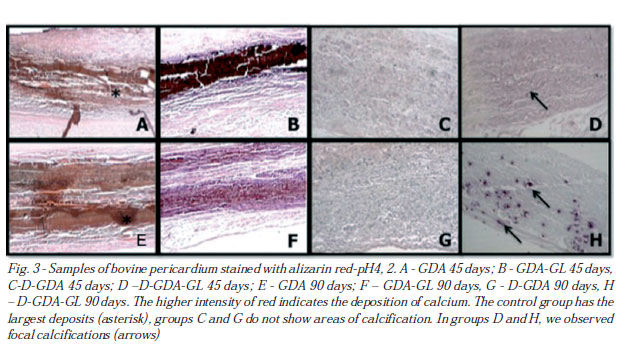
Staining with alizarin at pH 4.2 and 7, the authors emphasize the presence of calcification, especially in groups GDA and GDA-GL, with large amounts of calcium crystals visible in the central region of the pericardium explanted. The best results were obtained with the group D-GDA, in which the calcification was non-existent or minimal in both periods. The pericardia from group D-GDA-GL had histological appearance similar to the group D-GDA on day 45 of evolution, however, at 90 days, it was already possible to show some small focal granules of calcification. Figure 3 illustrates the histological aspects of staining with alizarin red pH 4.2, which show calcification due to deposition of crystals of calcium phosphate at 45 and 90 days of evolution.
Morphometry of the amount of calcium by alizarin staining at pH 4.2 and 7, confirmed the visual interpretation of histological images (Figure 4). Statistically, all groups had significantly less calcification than the control group. However, when compared group to group, group D-GDA was the one which statistically had the lowest rates of calcification at 45 and 90 days of evolution (P <0.0001) compared to other groups. The only exception was the group D-GDA-GL at 45 days, where calcification by alizarinred pH 7 was similar to group 3.

Quantitation of calcium
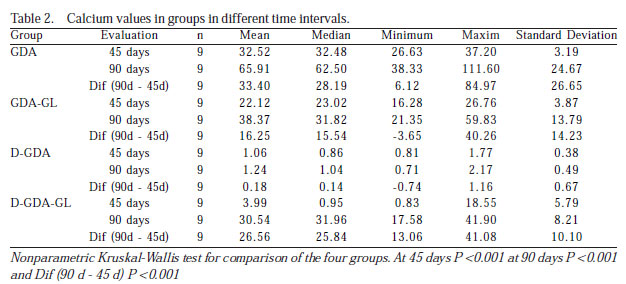
The values of the amount of calcium in ì g of calcium/mg of tissue obtained by atomic absorption spectrophotometry are shown in Table 2 and Figure 5.

It can be observed that the amount progressively increased in groups GDA, GDA-GL and D-GDA-GL. Similarly to what was observed by morphometry, all groups had significantly less calcification than the control group. The D-GDA group, in addition to being the one that had the lowest values for the amount of calcium was the only one who showed no calcification, with similar values at 45 and 90 days of evolution (P = 0.314). The comparison of the two by two groups in the time intervals can be seen in Table 3.

DISCUSSION
The mechanisms of calcification of biological valve prostheses are complex and multifactorial, involving biochemical, immunological and biomechanical aspects among others3. Furthermore, the interaction of biological factors related to patients with heterologous tissue after implantation are important in the occurrence of tissue degeneration and progressive dystrophic calcification [1-3].
It is well established that the membranes and cellular debris, rich in phospholipids are the source of initial deposition of calcium crystals. The combination of these crystals causes the formation of nodules with consequent thickening and thinning of the fabric, increasing the amount of dystrophic calcification. Furthermore, the inflammatory reaction caused by the presence of fixed tissue and the residual aldehyde fixation process, calcium eager to favor a gradual deposition of crystals [3-5].
Several therapeutic approaches have been tested in order to prevent or delay tissue degeneration, thus prolonging the durability of bioprostheses. These approaches aim to preferentially interfere with two main mechanisms of calcification: remove the elements capable of initiating tissue calcification or neutralize toxic aldehyde residuals resulting from tissue fixation solution [9].
The tissue decellularization technology for the use of detergent solutions and / or enzyme, has been employed in order to completely remove all cells and cellular debris, leaving only the extracellular matrix intact [14]. This methodology can be dual contribution to reducing calcification, and removes the cells as initial point of calcium deposition, reduces the antigenicity of the tissue, which might decrease the inflammatory and immune response by the recipient, which would tend to decrease the progressive tissue degeneration [16].
Our research group at the Center for Cardiovascular Grafts of PUCPR developed decellularization solution based on 0.1% SDS solution. This solution was initially tested in aortic and pulmonary homografts, and the results, both experimental and clinical, have demonstrated marked reduction in calcification [18,19]. Thus, it seemed appropriate to study the effects of this solution in heterologous tissues fixed in glutaraldehyde, to verify its effectiveness as an agent in calcification of bovine pericardial bioprostheses and / or porcine prostheses.
The efficiency of our method of decellularization was confirmed by histologic controls with HE performed before fixation with glutaraldehyde (Figure 1), where we observe the presence of an intact collagen extracellular matrix with a complete absence of cellular elements. Similar work had been done by Oswal et al. [15], demonstrating that SDS solution allowed the complete bovine pericardium decellularization of maintaining the integrity of the extracellular matrix.
We chose the model of subcutaneous implantation in rats, being a cheap, practical and well established in the literature. However, we are aware that, once proven the effectiveness of the methodology will be needed for confirmation in more sophisticated models, such as implantation in pulmonary or systemic circulation of sheep.
Preliminary study of our research group, using the same experimental model used here, has shown that glutamic acid was effective in reducing the calcification of bovine pericardium fixed in glutaraldehyde [12]. For this reason, fixed in glutaraldehyde bovine pericardium formed our control group, whereas the addition of decellularization or post-treatment were compared with glutamic acid alone or in combination to determine the most efficient way to reduce calcification.
The correlation between the intensity of the inflammatory response and the occurrence of calcification was demonstrated by Manjii et al. [4]. In our study, we found that all groups have caused some degree of inflammatory reaction, however, the group D-GDA was what the answer was more attenuated. Similar results were reported by Gonçalves et al. [16], which showed that removal of cells eliminates antigens present in the membranes, reducing the inflammatory foreign body of the heterograft. Wang et al. [6] used the tannic acid, reducing the inflammatory reaction, with consequent reduction in calcification of bovine pericardium. In our results with glutamic acid, we observed that the inflammatory reaction was similar to the control group. Furthermore, addition of glutamic acid treatment to decellularized pericardium (DGDA-GL) inflammatory response triggered steeper than the pericardium only decellularized (D-GDA). The explanation for this finding is not apparent, but we understand that the acidic pH of this treatment can somehow damage the fiber structure of the extracellular matrix, leading to greater intensity of inflammatory reaction.
By alizarin-red staining at pHs of 4.2 and 7.0, we observed that calcification had direct correlation with the intensity of the inflammatory reaction. The pericardium groups GDA and GDA-GL developed severe calcification occupying the entire central portion of the fabric, while the pericardium is decellularized showed calcification free, even after 90 days of development. Although the results in group D-GDA-GL are similar to those of group D-GDA 45 days thereafter we observed some focal calcification at 90 days, demonstrating that there was no synergism in the actions of anticalcification decellularization with glutamic acid.
The quantitative measurement of the amount of calcium confirmed our morphometric analysis. Treatment with glutamic acid reduced the amount of calcium in the control group, which had been documented by Ferreira et al. [12]. Moreover, the study of Jorge-Herrero et al. [8] glutamic acid was not as effective and, paradoxically, the pericardium treated behaved worse than the control group. Conflicting results from these studies can at least partly be explained by different methods in the use of glutamic acid, such as concentration, pH and temperature of exposure of the tissue.
The effectiveness of the decellularization method as calcification of bovine pericardium fixed in glutaraldehyde can be clearly demonstrated by the negligible amount of calcium found at 45 days (1.06 mg / mg tissue) and remained stable within 90 days of evolution (1, 24 ì g / mg tissue), these values being significantly lower than those found in other groups. As already evidenced by histological analysis, the post-treatment with glutamic acid in the pericardium was not decellularized anticalcification method as synergism. Instead, despite the calcium values were similar in groups D-GDA and D-GDA-GL at 45 days of evolution, the longer observation for 90 days showed a significant increase of calcium in the group D-GDA-GL. As demonstrated by Jorge-Herrero et al. [8], glutamic acid displays unstable connection with aldehydes residual GDA, which break through the passage of time, which would favor the formation of crystals of calcium at a later stage. The explanation for the possible deleterious effect of glutamic acid in this situation should be further understood.
Costa et al. [13] have demonstrated experimentally the effectiveness of the decellularization method as calcification in bovine pericardium. In this study, the decellularization of bovine pericardium using an alkaline solution to prevent calcification in 90 days. In the method of Shen et al. [7] with the combination of ethanol, ether and Tween 80 detergent, calcium levels were 13.1 ì g / mg tissue in mice at 180 days. In our study, the amount of calcium found in decellularized pericardium was low, with a reduction of 65 µg / mg tissue in the control group to 1.24 µg / mg tissue in the pericardium treated for 90 days of evolution. Although the results can not be directly compared due to differences in methodologies and varying times of observation, reducing the amount of calcium has been a common denominator in these studies. Furthermore, the efficiency of use of detergents such as SDS method as in heterologous tissue calcification can already be achieved clinically proven explants prosthesis Hancock II. In a study of Bottio et al. [17], the removal of phospholipids by SDS levels resulted in only 14.70 mg calcium / g tissue prostheses structural degeneration of explanted human versus 99 mg calcium / g of tissue calcification after prosthesis degeneration with an average 94 months of implantation in humans.
Other anticalcification methods, although reducing the amount of calcium, were not as effective as compared to decellularization. Wang et al. [6] observed a reduction of calcium levels of 90 mg / g tissue in the control group to 6.4 mg / g tissue at 21 days after surgery with the use of tannic acid. Since Pettenazzo et al. [9] demonstrated the effectiveness of using octanediol, with reduced levels of calcium of 165 µg / mg to 2.36 µg / mg at 75 days. Carpentier et al. [11], heat treatment at 50 º C, reduced calcium levels of 108 µg / mg of tissue to 19 mg / mg of tissue implants in rats for 90 days.
CONCLUSION
The decellularization of bovine pericardium with 0.1% SDS solution (Solution PUCPR) was effective in reducing calcification by up to 90 days in subcutaneous implants in rats. There was no further reduction in the amount of calcium by simultaneous treatment with glutamic acid. Based on these results, we recommend the confirmation of its effectiveness in a circulation model of large animals.
REFERENCES
1. Carpentier A, Lemaigre G, Robert L, Carpentier S, Dubost C. Biological factors affecting long-term results of valvular heterografts. J Thorac Cardiovasc Surg. 1969;58(4):467-83. [MedLine]
2. Schoen FJ, Levy RJ, Hilbert SL, Bianco RW. Antimineralization treatments for bioprosthetic heart valves. Assessment of efficacy and safety. J Thorac Cardiovasc Surg. 1992;104(5):1285-8. [MedLine]
3. Schoen FJ, Levy RJ. Calcification of tissue heart valve substitutes: progress toward understanding and prevention. Ann Thorac Surg. 2005;79(3):1072-80. [MedLine]
4. Manji RA, Zhu LF, Nijjar NK, Rayner DC, Korbut GS, Churchill TA, et al. Glutaraldehyde-fixed bioprosthetic heart valve conduits calcify and fail from xenograft rejection. Circulation. 2006;114(4):318-27. [MedLine]
5. Gross JM. Calcification of bioprosthetic heart valves and its assessment. J Thorac Cardiovasc Surg. 2001;121(3):428-30. [MedLine]
6. Wang D, Jiang H, Li J, Zhou JY, Hu SS. Mitigated calcification of glutaraldehyde-fixed bovine pericardium by tannic acid in rats. Chin Med J (Engl). 2008;121(17):1675-9. [MedLine]
7. Shen M, Kara-Mostefa A, Chen L, Daudon M, Thevenin M, Lacour B, et al. Effect of ethanol and ether in the prevention of calcification of bioprostheses. Ann Thorac Surg. 2001;71(5 Suppl):S413-6. [MedLine]
8. Jorge-Herrero E, Fernández P, Escudero C, García-Páez JM, Castillo-Olivares JL. Calcification of pericardial tissue pretreated with different amino acids. Biomaterials. 1996;17(6):571-5. [MedLine]
9. Pettenazzo E, Valente M, Thiene G. Octanediol treatment of glutaraldehyde fixed bovine pericardium: evidence of anticalcification efficacy in the subcutaneous rat model. Eur J Cardiothorac Surg. 2008;34(2):418-22. [MedLine]
10. Sardeto EA, Costa FDA, Costa ISEA, Roderjan JG, Discher E, Scheneider RA, et al. Eficácia do AlCl3 e etanol na prevenção da calcificação de fragmentos da parede aórtica porcina fixados em GDA. Rev Bras Cir Cardiovasc. 2006;21(4):409-17. View article
11. Carpentier SM, Chen L, Shen M, Fornes P, Martinet B, Quintero LJ, et al. Heat treatment mitigates calcification of valvular bioprosteses. Ann Thorac Surg. 1998;66(6 Suppl):S264-6. [MedLine]
12. Ferreira ADA, Costa FDA, Santos EAA, Sardeto EA, Gomes CHGG, Collatusso C, et al. Ácido L-glutâmico na prevenção da calcificação de pericárdio bovino fixado em glutaraldeído: estudo em ratos. Rev Bras Cir Cardiovasc. 2007;22(3):303-9. [MedLine] View article
13. Costa JNL, Pomerantzeff PMA, Braile DM, Ramirez VA, Goissis G, Stolf NAG. Comparação entre o pericárdio bovino decelularizado e o pericárdio bovino convencional utilizado na confecção de biopróteses valvares cardíacas. Rev Bras Cir Cardiovasc. 2005;20(1):14-22. View article
14. Gilbert TW, Sellaro TL, Badylak SF. Decellularization of tissues and organs. Biomaterials. 2006;27(19):3675-83. [MedLine]
15. Oswal D, Korossis S, Mirsadraee S, Wilcox H, Watterson K, Fisher J, et al. Biomechanical characterization of decellularized and cross-linked bovine pericardium. J Heart Valve Dis. 2007;16(2):165-74. [MedLine]
16. Gonçalves AC, Griffiths LG, Anthony RV, Orton EC. Decellularization of bovine pericardium for tissue-engineering by targeted removal of xenoantigens. J Heart Valve Dis. 2005;14(2):212-7. [MedLine]
17. Bottio T, Thiene G, Pettenazzo E, Ius P, Bortolotti U, Rizzoli G, et al. Hancock II bioprosthesis: a glance at the microscope in mild-long-term explants. J Thorac Cardiovasc Surg. 2003;126(1):99-105. [MedLine]
18. Costa FDA, Dohmen P, Vieira ED, Lopes SV, Collatusso C, Pereira EWL, et al. Operação de Ross com homoenxertos valvares descelularizados: resultados de médio prazo. Rev Bras Cir Cardiovasc. 2007;22(4):454-62. [MedLine]
19. Costa FD, Costa AC, Prestes R, Domanski AC, Balbi EM, Ferreira AD, et al. The early e midterm function of decellularized aortic valve allografts. Ann Thorac Surg. 2010;90(6):1854-60. [MedLine]
20. Maizato MJ, Pires MD, Canzian M, Higa OZ, Pitombo RN, Leirner AA. Histological evaluation of biocompatibility of lyophilized bovine pericardium implanted subcutaneously in rats. Artif Organs. 2008;32(4):268-71. [MedLine]
Article receive on Monday, October 3, 2011
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}