INTRODUCTION
Since the advent of cardiopulmonary bypass (CPB), also called perfusion, great benefits were acquired, when enabling appropriate conditions for the surgical correction of various heart diseases, temporarily replacing the functions of the lungs and heart. However, by altering human physiology, CPB can cause adverse effects such as hematological disorders and inflammatory reactions during and after use, mainly due to excessive hemodilution.
In an attempt to reduce the deleterious effects of hemodilution, several strategies implemented during the perfusion have been raised, which have been examined for their efficacy [2-4]. The most recent is the vacuum assisted venous drainage (VAVD), which is being used during cardiac surgery with CPB, aiming to optimize the venous drainage, as well as reduce the use of crystalloids in order to obtain higher values +of hematocrit [ 5].
VAVD technique is the use of negative pressure in the venous reservoir, allowing for active venous drainage, thus eliminating the principles of trapping and gravity, for example, it is possible to raise and shorten the entire CPB circuit and managing a smaller volume of crystalloid. That way, it can be obtained limited hemodilution, resulting in a possible lower incidence of blood transfusion [2,5].
The aim of this study was to report the experience with the technique of vacuum assisted venous drainage in cardiac surgery with cardiopulmonary bypass and verify the need for blood transfusion within this single group.
We studied 111 patients, of whom 64 (57.7%) males and 47 (42.3%) females, retrospectively by medical records of patients undergoing cardiac surgery with CPB and use of VAVD in the period of October 2006 to February 2008, at Hospital Esperança in Recife, Pernambuco. The age ranged from 11 to 88 years and averaged 59.50 ± 14.88 years, weighing between 40 and 107 kg (mean 69.18 ± 13.27 kg). We excluded all patients undergoing cardiac surgery of urgency, reoperation and those who had previously diagnosed bleeding disorders. This study was approved by the Ethics Committee of Fundação Altino Ventura under Protocol (CEP N.002/09 CEP/FAV).
The need for blood transfusion was compared within one study group, who used VAVD, and variables such as gender, weight and age of patients in the pre-CPB and perioperatively by the number of red blood cells used in order to evaluate possible associations with increased risk of blood transfusion.
According to the routine adopted by the service, blood transfusion was performed before the start of CPB when HT <33% or Hb <11 g/dl in CPB when HT <24% or Hb <8/ dl, and during the postoperative when HT <30% or Hb <10 g/dL.
VAVD
System We used the sealed membrane oxygenator, developed by NIPRO Medical-LTDA, Vital model - EDO 30 P, whose points of tube connections have blanking plugs that do not allow entry of air into the venous reservoir, when not being used. On the cover of the venous reservoir there is a safety valve that works like exhaust air to protect against excessive negative pressure. To adjust the vacuum pressure needed, we used a set of valves that regulate the negative pressure provided by the network, and compensate for fluctuations of the hospital network (Figure 1).

Fig. 1 - Set of valves that regulate the negative pressure provided by the network
The software used was SPSS for Windows version 12.0 (Chicago, IL). Univariate analysis was performed to identify if the variables, gender, age and weight alter the risk of the patient to need for transfusion in the pre-CPB, and during the perioperative period. We applied the Chi-Square Pearson test for qualitative variables and Student t test for quantitative ones.
For the quantitative measure the aim was to determine if the averages were similar between groups (using X transfusion without the use of transfusions). Prior to the tests of mean comparisons, an analysis was performed to test the hypothesis that the data followed a normal distribution. This type of testing helps to choose between parametric and nonparametric tests. This was performed by the Kolmogorov-Smirnov test. Like all quantitative variables, age and weight were normally distributed, we chose to use the Student t test for comparison between groups. The significance level was
P <0.05.
RESULTS
In 111 operated cases, the initial HT ranged from 22% to 48% (average 35.29%), falling during CPB between 18% and 39% (average 27.14%), while the post-HT operative period rose from 23.8% and 41.2% (average 33.4%).
In 100 (90%) patients, there was no need for blood transfusion before the start of the infusion, and only one unit of PRBC was used by 15 (13.5%) of the sample during CPB. The maximum number of PRBC units did not exceed three per patient at all times evaluated, and 39 (35.1%) patients required more than one unit of PRBC (CH) in the immediate postoperative period.
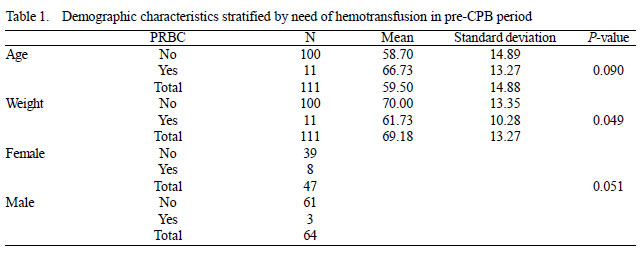
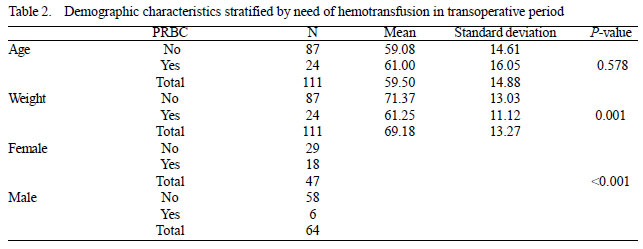
According to the results, there was no statistical difference (P=0.05) association between gender and use of blood in the pre-CPB, while it points the women with a higher percentage of transfusion compared with men (17% vs 4 7% respectively). Likewise, during surgery the women received more blood transfusion (38% vs 9% respectively), this time, with statistical difference (
P <0.001).
In Table 1, we find that among the quantitative variables, only weight were significant, and can state that the patients who did not pre-CPB transfusion weighed, on average, 8 kg more than those who were not transfused.
During surgery, the weight variable was also significant for patients with need for blood transfusion, indicating that they weighed on average 10 kg less. However, according to Table 2, it was observed that reached the age variable Pvalue <0.10 and could be included in the multivariate analysis, along with gender.
DISCUSSION
Thanks to technological advancements that now allow for the development of minimally invasive cardiac surgery, where the technique of VAVD has been essential safely and effectively [7-10], is also increasing the number of studies on the use of this technique in cardiac surgery of access and traditional cannulation. In this sense, these authors cite several benefits gained by the substitution of conventional drainage, which is based on sinfonagem and gravity drainage by using the active vacuum [11-17].
Reporting our experience with VAVD and need for blood transfusion in patients undergoing this technique, compared to gender, age and weight, was the main interest of this study, which showed a similar percentage of patients Blood transfusion in the pre-CPB (9.9 %) and during infusion (13.5%) to the numbers found by BANBURY et al [17], where 13% of patients receiving blood transfusions during CPB. These findings are consistent with other studies in the literature [11,12], even in pediatric cardiac surgery [13], which are few published articles.
A likely explanation for these results lies in the fact VAVD allows shortening the CPB circuit lines, along with higher placement of the membrane oxygenator, leading to a reduction of hemodilution induced by infusion, related to the low volume of crystalloid added to completing the circuit [11-13].
Laboratory research on dogs also point to the ability of simplification and miniaturization of the CPB circuit, venous drainage through the vacuum, resulting in limited production of hemoglobin and higher levels of hemoglobin, compared with operated animals with conventional venous drainage [5 ].
However, Pappalardo et al. [14] in a prospective randomized study, did not identify any significant difference in blood transfusion between both groups, although the group that underwent perfusion with VAVD has been transfused and has produced less hemoglobin and hematocrit were significantly higher. Given this, the authors suggest consideration of the technique, especially for patients with low weight, which would benefit most from the control of blood dilution.
According to this study, patients who needed blood transfusion during surgery weighed on average 80 to 10 kg less compared to those not transfused. This may indicate the need for greater care with this group of patients, translated by better planning of which technique to use, as well as strategies to avoid the use of red blood cells or reduce it to the maximum possible. However, studies on the use of VAVD decision based on the trial of the perfusionist in partnership with the surgeon, according to the criteria evaluated during the course of CPB, found a low percentage of patients with low weight and body surface in those who required the use of the technique [9].
Another clinical benefit reported in the literature refers to VAVD refers to efficient decompression cardiac surgery field by offering a more appropriate, as a result of venous drainage effective, regardless of positioning and handling of the heart [15-17]. Although this is an aspect more subjective, Münster et al. [16] reported that during the infusion technique VAVD less volume was added to the oxygenator, referring to times when there was difficulty with venous drainage, an average of 250 ml per patient against 1000 ml per patient in the control group.
Although women had a higher need for blood transfusion, according to the study, it is not possible to say that females behave as a factor that predisposes the use of blood alone because there are reports of women presenting hemoglobin levels lower in preoperative cardiac surgery, thus influencing the risk of blood transfusion [18]. Another reason that prevents such a conclusion is due to the fact that there is scarcity of scientific articles that explore the way the relationship between the investigative technique of VAVD, the need for blood and gender.
This study, being retrospective, had some limitations. One refers to its observational characteristic, albeit with an analytical component, which could not affect or define the shape and/or range of data collection on record. Another issue is related to the absence of a control group, not allowing comparison between groups, especially with the group without VAVD. However, the importance of the study is to report positive experience with the technique and point out some guidelines for further research on the subject, in view of the other findings of statistical analysis that showed a significant ratio of weight to the need for blood transfusion. Moreover, the results were very close to some comparative studies, which found a low incidence of the use of blood in cases submitted to VAVD technique.
Thus, one can conclude that the technique has been used in a useful and satisfactory manner in helping to venous drainage during CPB, in the service that performed the survey, but it lacks information on the possible reduction in the need for blood transfusion that allows its application, especially having to be assessed the influence of some factors such as initial hematocrit level and gender, when starting from the same levels through future prospective investigations and comparative with the conventional CPB to further elucidate these issues.
REFERENCES
1. Gravlee GP, Davis RF, Utley JR. Cardiopulmonary bypass: principles and practice preface. 3ª ed. Baltimore:Williams & Wilkins;2008.
2. Canêo LF, Lourenço Filho DD, Rocha e Silva R, Jatene FB, Turri F, Leirner AA. Drenagem venosa assistida através da utilização controlada de vácuo no reservatório venoso do oxigenador. Rev Bras Cir Cardiovasc. 1999;14(2):135-8.
3. Souza DD, Braile DM. Avaliação de nova técnica de hemoconcentração e da necessidade de transfusão de hemoderivados em pacientes submetidos à cirurgia cardíaca com circulação extracorpórea. Rev Bras Cir Cardiovasc. 2004;19(3):287-94.
4. Souza HJB, Moitinho RF. Estratégias para redução do uso de hemoderivados em cirurgia cardiovascular. Rev Bras Cir Cardiovasc. 2008;23(1):53-9.
5. Taketani S, Sawa Y, Masai T, Ichikawa H, Kagisaki K, Yamaguchi T, et al. A novel technique for cardiopulmonary bypass using vacuum system for venous drainage with pressure relief valve: an experimental study. Artif Organs. 1998;22(4):337-41.
6. Alghamdi AA, Davis A, Brister S, Corey P, Logan A. Development and validation of Transfusion Risk Understanding Scoring Tool (TRUST) to stratify cardiac surgery patients according to their blood transfusion needs. Transfusion. 2006;46(7):1120-9.
7. Kiyama H, Imazeki T, Katayama Y, Murai N, Mukouyama M, Yamauti N. Vacuum-assisted venous drainage in single-access minimally invasive cardiac surgery. J Artif Organs. 2003;6(1):20-4.
8. Colangelo N, Torracca L, Lapenna E, Moriggia S, Crescenzi G, Alfieri O. Vacuum-assisted venous drainage in extrathoracic cardiopulmonary bypass management during minimally invasive cardiac surgery. Perfusion. 2006;21(6):361-5.
9. Murai N, Cho M, Okada S, Chiba T, Saito M, Shioguchi S, et al. Venous drainage method for cardiopulmonary bypass in single-acces minimally invasive cardiac surgery: siphon and vaccum-assisted drainage. J Artif Organs. 2005;8(2):91-4.
10. Shin H, Yozu R, Maehara T, Matayoshi T, Morita M, Kawai Y, et al. Vacuum assisted cardiopulmonary bypass in minimally invasive cardiac surgery: its feasibility and effects on hemolysis. Artif Organs. 2000;24(6):450-3.
11. Hayashi Y, Kagisaki K, Yamaguchi T, Sakaguchi T, Naka Y, Sawa Y, et al. Clinical application of vacuum-assisted cardiopulmonary bypass with a pressure relief valve. Eur J Cardiothorac Surg. 2001;20(3):621-6.
12. Borrelli U, Al-Attar N, Detroux M, Nottin R, Nikis S, Jennes S, et al. Compact extracorporeal circulation: reducing the surface of cardiopulmonary bypass to improve outcomes. Surg Technol Int. 2007;16:159-66.
13. Nakanishi K, Shichijo T, Shinkawa Y, Takeuchi S, Nakai M, Kato G, et al. Usefulness of vacuum-assisted cardiopulmonary bypass circuit for pediatric open-heart surgery in reducing homologous blood transfusion. Eur J Cardiothorac Surg. 2001;20(2):233-8.
14. Pappalardo F, Corno C, Franco A, Giardina G, Scandroglio AM, Landoni G, et al. Reduction of hemodiluition in small adults undergoing open heart surgery: a prospective, randomized trial. Perfusion. 2007;22(5):317-22.
15. Bevilacqua S, Matteucci S, Ferrarini M, Kacila M, Ripoli A, Baroni A, et al. Biochemical evaluation of vacuum-assisted venous drainage: a randomized, prospective study. Perfusion. 2002;17(1):57-61.
16. Munster K, Andersen U, Mikkelsen J, Pettersson G. Vaucum assisted venous drainage (VAVD). Perfusion. 1999;14(6):419-23.
17. Banbury MK, White JA, Blackstone EH, Cosgrovo DM 3rd. Vacuum-assisted venous return reduces blood usage. J Thorac Cardiovasc Surg. 2003;126(3):680-7.
18. Dial S, Delabays E, Albert M, Gonzalez A, Camarda J, Law A, et al. Hemodilution and surgical hemostasis contribute significantly to transfusion requirements in patients undergoing coronary artery bypass. J Thorac Cardiovasc Surg. 2005;130(3):654-61.
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket