CLINICAL DATA
9-year-and-6-month child, 37.4 kg, female, from Colômbia, São Paulo State. She did not present signs or symptoms - aside from the ignored complaint to the family of a "sensation of chest tightness" that improved with deep breathing. In a routine medical consultation (after patient came down with tonsillitis) irregular cardiac auscultation was revealed, and an echocardiogram was requested, revealing congenital heart disease with pulmonary hyperflow.
Her physical examination upon admission into our practice was relatively normal; she presented with good general condition, eutrophic, afebrile and acyanotic. We noticed only regular heart rhythm without murmurs, with fixed doubling of second heart sound (more audible at a pulmonary focus).
ELECTROCARDIOGRAM
Sinus rhythm, heart beat of 88 bpm, SÂP 0°, SÂQRS +120°, PR 160s, QRS 80s. Right ventricle overload (RV), right QRS axis deviation at V1 and notched R-wave with 13mm amplitude (Figure 1).
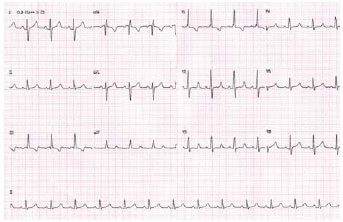
Fig. 1 - Electrocardiogram showing little interatrial communication
Visceral
situs solitus with levocardia. Normal heart area with normal cardiothoracic index of 0.53. Pulmonary vascular network unchanged, free diaphragmatic domes (Figure 2).
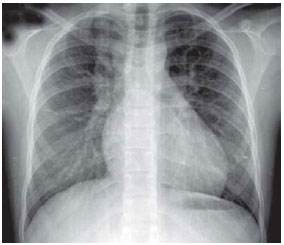
Fig. 2 - Chest radiography without significant changes indicating interatrial communication
with levocardia. The venoatrial, atrioventricular and ventriculo-arterial connections were all normal. Doppler detected interatrial septum with minimal flow entering into the right atrium (RA) compatible with
ostium secundum-type interatrial communication and turbulent systolic flow in the RA, indicating slight tricuspid insufficiency. The RV systolic pressure was 40 mmHg. The pulmonary to systemic blood flow ratio (Qp/Qs) estimation was 3,3:1, with interatrial communication measuring up to 20mm and severe hemodynamic repercussion.
DIAGNOSIS
It is common for children in our clinics to not present signs and symptoms of heart disease. Often, these children practice physical activities and usually their parents have problems believing in the pre-existence of the disease.
Few clinical symptoms is often characteristic of interatrial communication without murmurs, and the electrocardiogram and chest rediography seem clear. The investigation must be appropriate and the operation must be indicated according to hemodynamic repercussion (QP/QS 1.5:1 or more) preferably between the ages of 3 and 4, in order to avoid several injuries to the heart and lungs [1,2 ].
OPERATION
Median transsternal thoracotomy, opening of the pericardium; we observed distention of the right chambers and dilation of pulmonary trunk (Fig. 3). We initiated conventional cardiopulmonary bypass (CPB) circuit using cannulas in the aorta and vena cava.
While still at normal body temperature, the aorta was clamped, the RA was opened, and aspiration for decompression of cavities was performed, as well as single anterograde hypothermic blood cardioplegia at 4ºC.
The edges of the interatrial septal defect (Figure 4) are identified. Sutures were used at the inferior edge (near the inferior vena cava). We used a 5-0 polypropylene continuous suture, closing up the orifice of the defect with a bovine pericardium patch (Figure 5).
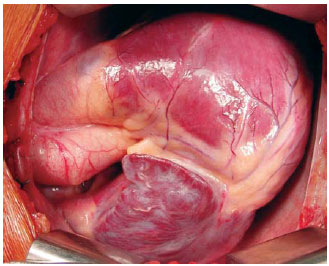
Fig. 3 - Right chamber distension after pericardium opening
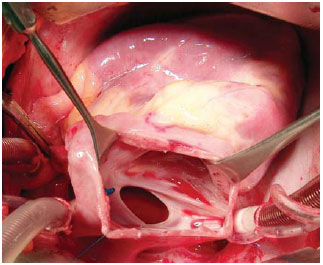
Fig. 4 - Opened right atrium showing large ostium secundum-type interatrial communication
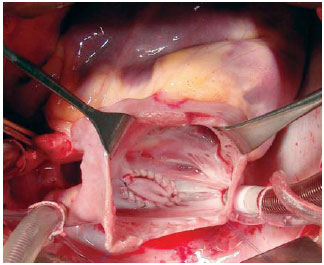
Fig. 5 - Opened right atrium with ostium secundum-type interatrial communication corrected with bovine pericardium patch
The patient was monitored in the ICU for 48 hours. Drains and central catheter were removed and the patient was referred to the recovery ward. She was discharged from the hospital on the fourth postoperative day, with a control echocardiography showing the correction of the defect.
REFERÊNCIAS
1. Christensen DD, Vincent RN, Campbell RM. Presentation of atrial septal defect in the pediatric population. Pediatr Cardiol. 2005;26(6):812-4. [
MedLine]
2. Muta H, Akagi T, Egami K, Furui J, Sugahara Y, Ishii M, et al. Incidence and clinical features of asymptomatic atrial septal defect in scool children diagnosed by heart disease screening. Circ J. 2003;67(2):112-5. [
MedLine]
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket