INTRODUCTION
Intracardiac primary tumors are rare conditions. About 75% of them are benign, and approximately 50% are myxomas. The symptoms are atypical and highly variable. According to the size and location of tumors, the patients may present symptoms that range from asymptomatic to a presentation of lung congestion, and may also present sudden death by thrombo-embolic phenomena. In this report, we present a case of an oligosymptomatic patient who underwent cardiological propaedeutic, which revealed a large left intra-atrial lesion. The patient then underwent surgical resection of this lesion. The anatomic-pathological study confirmed the diagnosis of myxoma. The patient developed pleural effusion in the postoperative, possibly related to the lesion.
CASE REPORT
63-year-old female patient who underwent cardiological evaluation due to dyspnea during medium effort, palpitation and precordialgia. During the examination, the patient presented as normotensive, with normal heartbeat, rhythmic and normophonetic sounds, without murmurs. ECG was normal. The chest X-Ray showed slight increase in the cardiac area. The patient did not present pre-existing diseases and did not use drugs regularly. She underwent an echocardiogram that showed a large mass in the left atrium, characterized by computed tomography as a great expansive ovoid lesion measuring 6.2 x 5.0 x 4.5 cm, and blocking a great part of the left atrial cavity with density slightly lower than the heart muscle.
The catheterization showed a large negative image in the left atrium (Fig. 1), and normal coronaries, as well as left ventricle with preserved contractility and mild venocapillary and arterial hypertension.
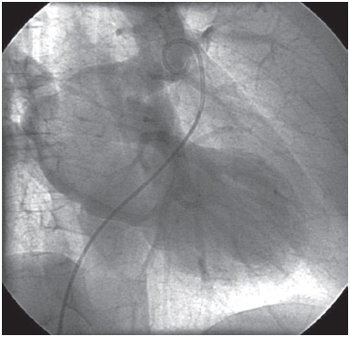
Fig. 1 - Catheterization: Large left atrial myxoma
The patient underwent surgical treatment with the use of cardiopulmonary bypass (CPB). After median sternotomy, cannulation of the aorta and cavas, aortic clamping and infusion of normothermic blood cardioplegic solution in the aortic root, a left atriotomy was performed, revealing a large mobile mass tumor, clear, with gelatinous consistency, friable with pediculated rooting in the high interatrial septum. The lesion was resected, and during the surgery, special care was taken to prevent its fragmentation. Its region of rooting was submitted to electrocauterization. The CPB suspension was routinely performed after the spontaneous return of the heartbeats.
The resected material was sent for anatomic-pathological study, which revealed that it was a smooth nodular mass, white-brownish, measuring 8.0 x 5.5 x 4.0 cm. The microscopy revealed the presence of stellate and globose cells arranged in myxoid stroma without severe atypias and with regular vascularization. The patient was discharged from the ICU on the 2nd postoperative day and from the hospital on the 16th postoperative day. The patient presented only bilateral pleural effusion on the 9th day of surgery, and needed thoracentesis for relief. The effusion showed good evolution after the procedrue. The control echocardiogram in the postoperative showed no atrial masses, the left atrium with a diameter within normal limits, and normal biventricular systolic function (Fig. 2).
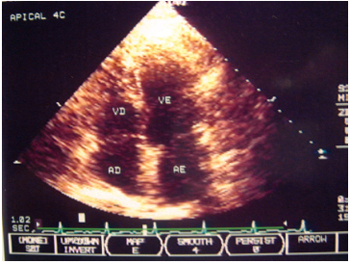
Fig. 2 - Echocardiogram on the 20th postoperative day
Among primary heart tumors, myxomas are the most frequent and represent about 50% of benign tumors [1]. Myxomas are real tumors. Ultrastructural examinations suggest that they are structures that arise from multipotent mesenchymal cells with endothelial derivation. Although these tumors present benign characteristics from the histological point of view, they may present unfavourable evolution due to their location, which is characterized by thromboembolic phenomena and may even lead to sudden death [2].
These tumors are located in the left atrium (LA) in approximately 75% of the cases [2], where they are almost always presented with signs and symptoms of mitral valve disease or thromboembolic events. They may also arise in other locations, such as aorta, pulmonary artery, ventricles, vena cavae or in other organs [3].
In about 50% of the cases, the tumor forms pediculated to the interatrial septum, but may have multiple focuses or may also cover the valvar tissue. The location, size and mobility of the tumors determine the clinical manifestations [4]. The propaedeutic methods used in the diagnosis of intracardiac myxomas ranged over decades. Before the advent of echocardiography, the atrial myxomas were suspected in patients who presented clinical signs of mitral stenosis, with a short time of evolution, without a prior history of rheumatic disease, with sinus rhythm, but with dyspnea or diastolic murmur (which may vary in supine position), and the patients were referred to surgery, which allowed for the correct diagnosis.
Currently, we can rely on echocardiography, including the three-dimensional echocardiography with the use of transesophageal transducers, with better structural cardiac definition, with both used in pre- or postoperative [5]. The first attempt at surgical resection was performed by Bahnson and Newman in 1952 and the first successful resection was performed by Crafoord in 1954. Generally, the surgical treatment is definitive and recurrence is unusual.
In this study, we found a case that was difficult to diagnose, due to the small amount of signs and symptoms. The patient was oligosymptomatic, with recent initiation of dyspnea during medium efforts, palpitation and mild precordialgia. The diagnosis was established using image methods (echocardiography, computed tomography and cardiac catheterization, which was also performed for a coronariographic study due to complaints of precordialgia), and revealed a myxoma of large dimensions. The patient underwent surgery (without complications) and an anatomic-pathological study confirmed that it was myxoma. In the postoperative, the patient presented the following complication: a rare association (already described) of bilateral pleural effusion possibly related to the myxoma [6].
REFERENCES
1. Lammer RJ, Bloor CM. Pathology of cardiac tumors. In: Kapoor AS, ed. Cancer of the heart. New York:Springer-Verlag;1986.
2. Bjessmo S, Ivert T. Cardiac myxoma: 40 year's experience in 63 patients. Ann Thorac Surg. 1997;63(3):697-700. [
MedLine]
3. Stolf NAG, Benício A, Moreira LFP, Rossi E. Mixoma de átrio direito com origem na veia cava inferior: uma localização rara com implicações diagnósticas e terapêuticas. Rev Bras Cir Cardiovasc. 2000;15(3):255-8.
4. Centofanti P, Di Rosa E, Deorsola L, Dato GM, Patanè F, La Torre M, et al. Primary cardiac tumors: early and late results of surgical treatment in 91 patients. Ann Thorac Surg. 1999;68(4):1236-41. [
MedLine]
5. Vieira MLC, Ianni BM, Mady C, Encinas J, Pommerantzeff PMA, Fernandes PP, et al. Mixoma de átrio esquerdo. Avaliação ecográfica tridimensional. Arq Bras Cardiol. 2004;82(3):281-3. [
MedLine]
6. Meira EBS, Camacho RG, Meira DBS, Povoa R, Kassab KK, Anijar AM, et al. Mixoma de átrio esquerdo associado a derrame pleural. Rev Bras Cir Cardiovasc 2000;15(3):259-62.
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket