CLINICAL DATA
We present a 14-year, 10 month-old-girl with Down syndrome, weighing 38 kg, born in Paraníba - MS - Brazil. At the age of 2 months, she begun to develop pneumonia and thought to have heart disorder. Due to socioeconomic difficulties she was referred to another medical center and heart disorder was confirmed only when she was 2-year, 8-month-old. At this time, she presented with continued fever, however without a clinical presentation of heart failure and/or cyanosis, and without medication, when suddenly she had a cardiorespiratory arrest of unknown cause. From this moment forth, she was treated with digoxin until the age of 7, when the family on its own account has decided to discontinue the medication. In January 2007, she was referred to our medical service with a classical clinical presentation of cardiac tamponade, which was surgically drained. At the time, congenital heart disease diagnosis was confirmed by echocardiogram and a significant lethargy was noted. Despite T3, T4, and TSH levels do not clearly indicate hypothyroidism, thyroxine sodium was the drug of choice. After 6 months, the clinical presentation course had a significant improvement and the patient was eupneic, hydrated, anicteric, with systolic murmur +/+6 in the left lower sternal border and a fixed splitting of S2. Heart rate was 100 bmp. Abdomen without tenderness on palpation and liver located 2 cm from the right costal margin. Radial and femoral pulses were normal.
ELECTROCARDIOGRAM
Electrocardiogram evidenced: sinus rhythm rate of 94 bmp; ÂP +60º, ÂQRS -60ºC; PR interval, 0.45 sec; QTc, 0.50 sec; QRS, 0.08 sec; left atrial and right ventricular overload; anterior division of de left bundle branch block, and first-degree AV block (Figure 1).
Fig. 1 - Electrocardiogram showing right ventricular and left atrial overload, anterior division of de left bundle branch block, and first-degree AV block
An overpenetrated X-ray view showed scoliosis of the thoracic segments of the vertebral column. The radiogram revealed visceral situs solitus heart. There was an increase in the cardiac area with a cardiothoracic index of 0.59, and the second aortic arch was dilated. It was also noted a pulmonary vascular prominence with vascular network inversion suggesting venocapillary hypertension (Figure 2).
Fig. 2 - Chest roentgenography showing the increase of cardiac area and pulmonary hyperflow signs
Situs Solitus was present at levocardia. The echocardiogram showed ostium secundum interatrial communication (IAC) with hemodynamic repercussion, 16 mm long, inferior vena cava and hepatic veins dilation without respiratory variability to Doppler. Moderate mitral insufficiency was noted. The estimate pulmonary-to-systemic flow ratio (QP/QS) was 2:1. Right ventricular systolic pressure was 31 mmHg; diameter of the aorta was 28 mm; left atrial diameter was 37 mm; right ventricular diameter 28 mm; left ventricular diameter was 37; right ventricular diastolic diameter was 28 mm; left ventricular diastolic diameter was 41 mm; left ventricular systolic diameter was 23 mm; "D de 43.9; and ejection fraction was 75.6%.
DIAGNOSIS
Patient's clinical history reminds us of the huge management difficulty faced by the socially less-favored patients with congenital heart disease in Brazil. The clinical information of continued fever, commonly seen in patients with Down syndrome, did not help the diagnosis. After so many years, congenital heart defect corrective surgery in a patient overage that has undergone prior pericardial drain surgery can be safely performed. It is important to highlight the need to adequate thyroid hormone levels in order to submit the patient to cardiopulmonary bypass. Thus, regarding the interatrial communication diagnosis, it was important to identify the clinical repercussion degree caused by the congenital heart disease and the hormonal deficit degree of origin and so finding the best time to recommend the surgery [1].
OPERATION
Median transsternal thoracotomy was performed with dissection of previous adhesions due to pericardial drainage. Cardiopulmonary bypass (CBP) support was established with normothermia and using unique hypothermic and anterograde blood cardioplegia. The right atrium was opened and an atrial septal defect was found to have a significant failure in formation and fenestration of oval fossa, thus characterizing ostium secundum interatrial communication (IAC) (Figure 3). Once the tendinous cords were resected, the mitral valve, which presented a subtle anterior cusp prolapse, was tested with saline solution and found competent. Interatrial communication was corrected with bovine pericardial patch and with running sutures of 4-0 polypropylene thread. Air was withdrawn from the cavities and the closure of the right atrium was concluded in the conventional way. Cardiopulmonary bypass and myocardial ischemia times were 25 minutes and 11 minutes, respectively. Hypothyroidism control was done postoperatively and the echocardiogram showed the following: subtle mitral regurgitation without hemodynamic repercussion; preserved myocardial contractility; and normal ejection fraction. Patient was discharge at postoperative day 6 using diuretic agent and thyroxine sodium.
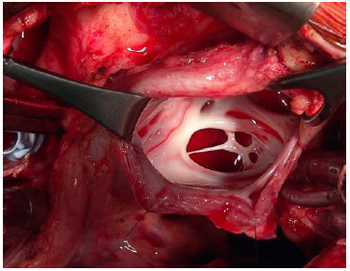
Fig.3 - Ostium secundum interatrial communication (IAC) with a fenestrated oval fossa
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket