INTRODUCTION
Pectus excavatum is a relatively common chest wall deformity in children. Numerous manuscripts in the literature does exist that document a variety of techniques available to repair pectus excavatum deformity with excellent cosmetic results [1-4].
However, the ideal age for correction of this defect is under considerable debate regarding the use of vertical or horizontal incision, and whether in the presence of a congenital heart defect the operation should be performed simultaneously or isolated [5-7].
The present study is to report a simultaneous operation to correct interatrial communication through atrioseptoplasty (with extracorporeal circulation) and repair of pectus excavatum through a longitudinal incision.
CASE REPORT
An 8-year-old male patient was referred to with clinical and echocardiographic diagnosis of ostium secundum-type interatrial communication, with moderate hemodynamic repercussion. Chest wall inspection revealed pectus excavatum-type anatomical deformity (Figure 1), which was confirmed by plain chest radiography (Figure 2).

Fig. 1 - Pectus excavatum-type deformity

Fig. 2 - Chest plain radiography
Aiming at to assess the severity of this deformity, a chest CT scan was performed to calculate the Haller index, which is used to determine the correlation between anterior and transverse chest diameters. A Haller index of 4.3 was obtained. Haller index greater than 3.25 indicates greater severity level of deformity and requires surgical repair (Figure 3) [7].
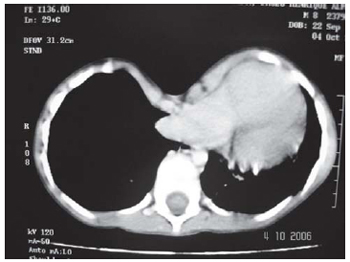
Fig. 3 - Chest Computerized Tomography
Initially, the operation technique comprised the correction of intracardiac defect. Median sternotomy and systemic heparinization (4 mg/kg) were performed with extracorporeal circulation (cardiopulmonary bypass) (by cannulation of ascending aorta and of both venae cavae). The correction of interatrial communication was performed via right atrium with bovine pericardium patch sutured to the border of the defect. The operation was performed at normothermia using as protective myocardial method the controlled hypoxia with i9ntermittent aortic clamping. After the atrioseptoplasty and the removal of extracorporeal circulation, with heparin reversion, the chest deformity was, finally, initiated.
The operation of pectus excavatum was performed by chondrosternoplasty, from the 4th to the 8th costal arches, subperichondrially and bilaterally according to the technique proposed by Robicsek et al. [8]. After the removal of these bone fragments, the sternum was fractured in the depressed point and then fixed parallel, thus correcting the anatomical deformity. The removal of the costal cartilage allows an easy displacement of the anterior chest wall, which after the sternal fracture can be correctly aligned (Figure 4) [9].
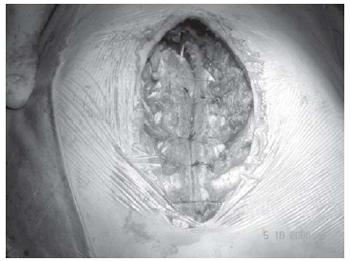
Fig. 4 - Parallel fixation of the fractured sternum in the depressed point after the resection of the costal arches
At the end of the operation (Figure 5), the patient in normothermia was referred to the postoperative unit, where he was continuously monitored.

Fig. 5 - Final aspect
The presence of a congenital intracardiac defect associated to pectus excavatum-type chest wall deformity showed an incidence varying between 0.17 and 0.50% of the cases and yet poses a dilemma for the surgeon [8]. Pectus excavatum can yield a shift in the heart's normal position, making the median sternotomy an access pathway, at times, unsatisfactory to simultaneously correct the intracardiac defects [1]. So, some authors have proposed to perform the operation separately due to the concern with a greater incidence of hemorrhagic complications, sternal infection and/or longer operative time [9].
However, in 1997, Willekes et al. [10] reported a low incidence of complications in 9 patients who underwent simultaneous pectus deformity repair.
Another favorable argument to perform the repair of both defects on the same operation is related to the compression of the heart structures after the congenital abnormality repair, with a consequently negative hemodynamic impact in these patients.
Several technical modifications were introduced in order to obtain the most possible bone stabilization, reducing the feasibility of this deformity recurrence in the post-operative course [5].
One possible alternative to correct pectus excavatum adds a longitudinal or transversal sternal split, with mobilization or resection of the deformed cartilages, without using a metal bar for sternal stabilization [6, 8].
Another approach involves the use of metal bars beneath the sternum for a 6-month period, and those who advocate this technique have suggested greater bony stability ion the immediate postoperative associated with a lower pain intensity [10].
It is worth mentioning that regardless the technique chose to perform the pectus deformity repair, the viability of the sternum can be maintained by preserving both internal thoracic arteries.
Another controversial factor is the ideal age to perform the pectus excavatum deformity repair, mainly by the possibility of deformity recurrence, especially in those patients under 4 years of age. So, in cases of early operation, it is recommended the removal of a limited number of costal cartilages, avoiding suturing the remaining perichondrium around the sternum.
In some cases, the presence of pectus excavatum may not allow the adequate access to the intracardiac structures due to the difficulty to place the sternal retractor, when the access pathway is the median sternotomy. In the operation performed in our institution, this pathway has allowed the adequate access to the heart. Besides, the technique chosen to repair the pectus excavatum deformity showed a satisfactory initial cosmetic result, once the technique employed can be followed by recurrence of the anatomical abnormality.
There was no difficulty to control the pain and the restrictive respiratory complication in the postoperative, as well. The patient was discharged 7 day after admission in good health conditions and will remain on outpatient follow-up.
So, in spite of being an isolated case, the initial result was satisfactory and the long-term outcome will confirm the viability of this technique in the absence of thoracic deformity recurrence.
REFERENCES
1. Okamura T, Nagase Y, Mitsui F, Shibairi M, Utsumi K, Watanabe H. Simultaneous repair of pectus excavatum and congenital heart defect in adults by using the convex bar. Ann Thorac Surg. 2004;77(5):1827-9. [
MedLine]
2. Haller JA Jr, Scherer LR, Turner CS, Colombani PM. Evolving management of pectus excavatum based on a single institutional experience of 664 patients. Ann Surg. 1989;209(5):578-82.
3. Kowalewski J, Brocki M, Zolynski K. Long-term observation in 68 patients operated on for pectus excavatum:surgical repair of funnel chest. Ann Thorac Surg. 1999;67(3):821-4. [
MedLine]
4. Golladay ES, Wagner CW. Pectus excavatum: a 15-year perspective. South Med J. 1991;84(9):1099-102. [
MedLine]
5. DeLeon MM, Magliato KE, Roughneen PT, Graham L, Kudukis TM, DeLeon SY. Simultaneous repair of pectus excavatum and congenital heart disease. Ann Thorac Surg. 1997;64(2):557-9. [
MedLine]
6. Jones WG, Hoffman L, Devereux RB, Isom OW, Gold JP. Staged approach to combined repair of pectus excavatum and lesions of the heart. Ann Thorac Surg. 1994;57(1):212-4. [
MedLine]
7. Haller JA Jr, Kramer SS, Lietman SA. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987;22(10):904-6. [
MedLine]
8. Robicsek F, Daugherty HK, Mullen DC, Harbold NB Jr, Hall DG, Jackson RD, et al. Technical considerations in the surgical management of pectus excavatum and carinatum. Ann Thorac Surg. 1974;18(6):549-64. [
MedLine]
9. Hasegawa T, Yamaguchi M, Ohshima Y, Yoshimura N, Oka S, Ootaki Y. Simultaneous repair of pectus excavatum and congenital heart disease over the past 30 years. Eur J Cardiothorac Surg. 2002;22(6):874-8. [
MedLine]
10. Willekes CL, Backer CL, Mavroudis C. A 26-year review of pectus deformity repairs, including simultaneous intracardiac repair. Ann Thorac Surg. 1999;67(2):511-8. [
MedLine]
 All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license
All scientific articles published at www.bjcvs.org are licensed under a Creative Commons license













 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket